24.6.21
Baljit Kaur 65 years old female

A detailed history of this patient’s journey towards several abdominal operations:
- Laparotomy (in PGI) in 1988 following enteric perforation of ileum resulting in peritonitis. The incision was long midline and vertical.
- 1992: the laparotomy was followed by an incisional hernia through that laparotomy incision; this was repaired possibly without a mesh in PGI again.
- 1996: an open cholecystectomy for gallstones was performed in Chandigarh government hospital sector 16, and they were told they also repaired through the same incision the incisional hernia which had recurred.
- 2000: An abdominal hysterectomy was performed (Shalley hospital) through the lower abdominal transverse (Pfannenstiel) incision.
- and 6. June/July 2021. The two surgeries given below starting with the incisional hernia first; and then
- a laparotomy for intestinal obstruction ending with resection of a big mass of matted small intestine which had been causing obstruction.
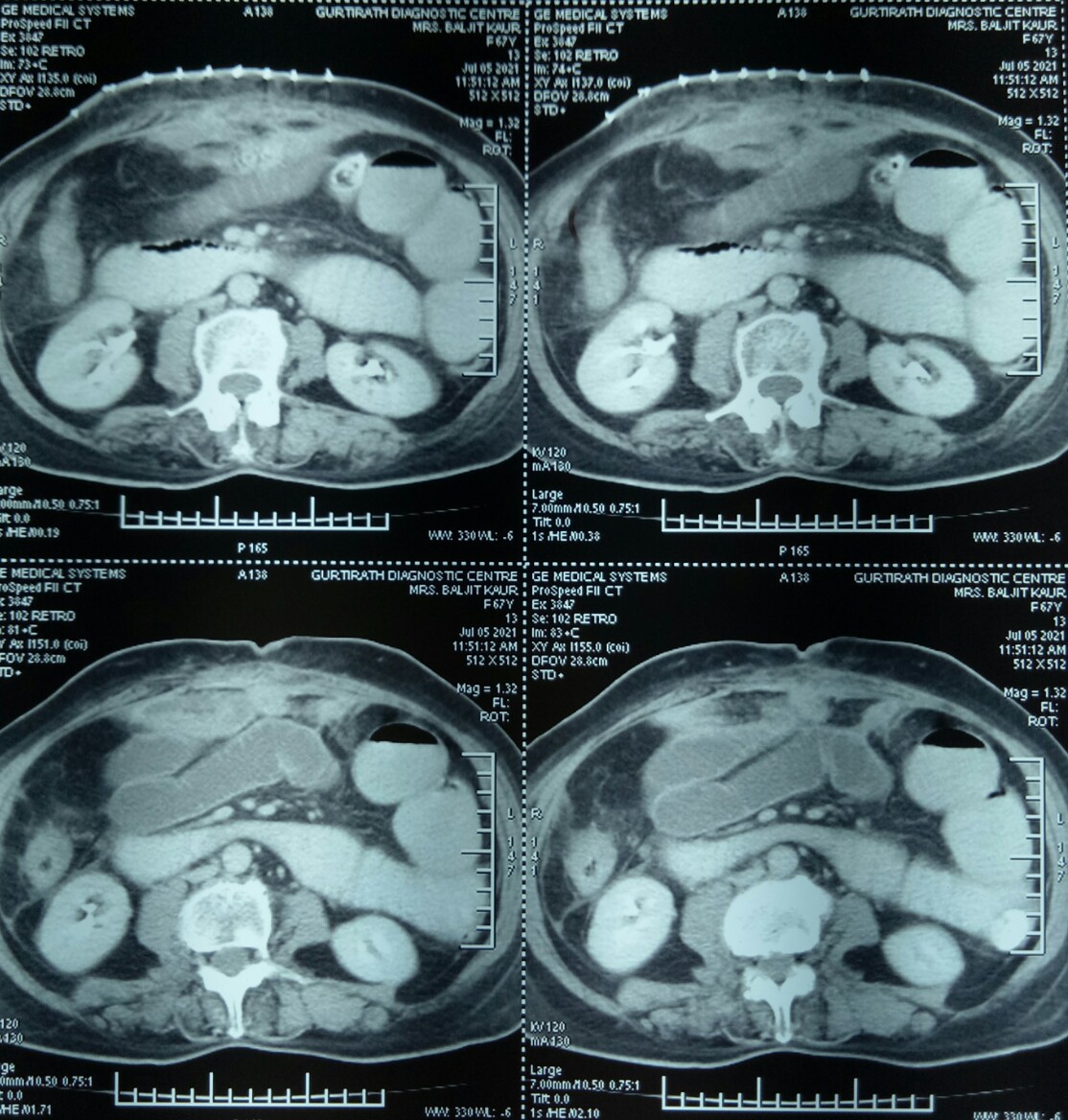
An incisional hernia (that had recurred perhaps for the third time) in the right upper part of the abdomen repaired in a 65 years old female. Because of the history of multiple operations earlier, a CT scan was performed and showed a defect in the anterior abdominal wall with a loop of intestine protruding.

Presuming it to be a routine case of an incisional hernia where the intestinal loop will be reduced back into the peritoneal cavity and the defect repaired, we started happily. But it turned out to be a nightmare when the loops of intestine just could not be separated from the edges of hernial defect, and it was discovered that some of these loops of small bowel were trapped in the prolene sutures used for the hernia repair earlier.
Diligently and slowly (taking nearly 3 hours, so as not to end up in a perforation) the intestinal loops were freed as much as possible through this incision and the hernia defect then defined after repositing the loops into the peritoneal cavity. The defect was then repaired with prolene sutures and a prolene mesh.
Postoperatively the patient seemed to be making good recovery for the first 3-4 days but then started having distension and vomiting, suggesting intestinal obstruction which did not respond to conservative treatment.
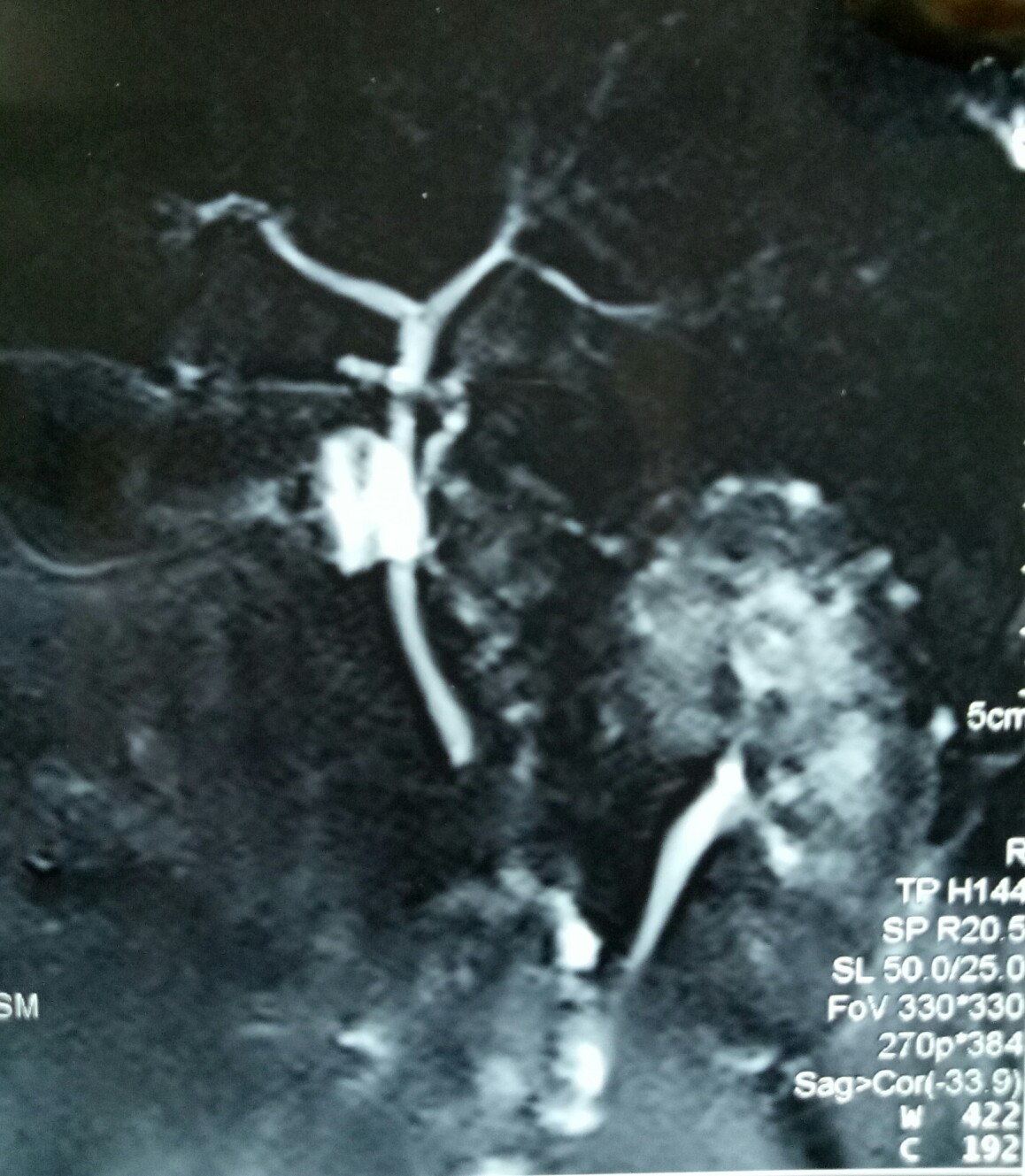
CT scans confirmed grossly dilated small bowel loops in the pelvis and left flank and one jejunal loop high in the centre, besides showing a mass of dense adhesions just under the staple line of the hernia surgery.

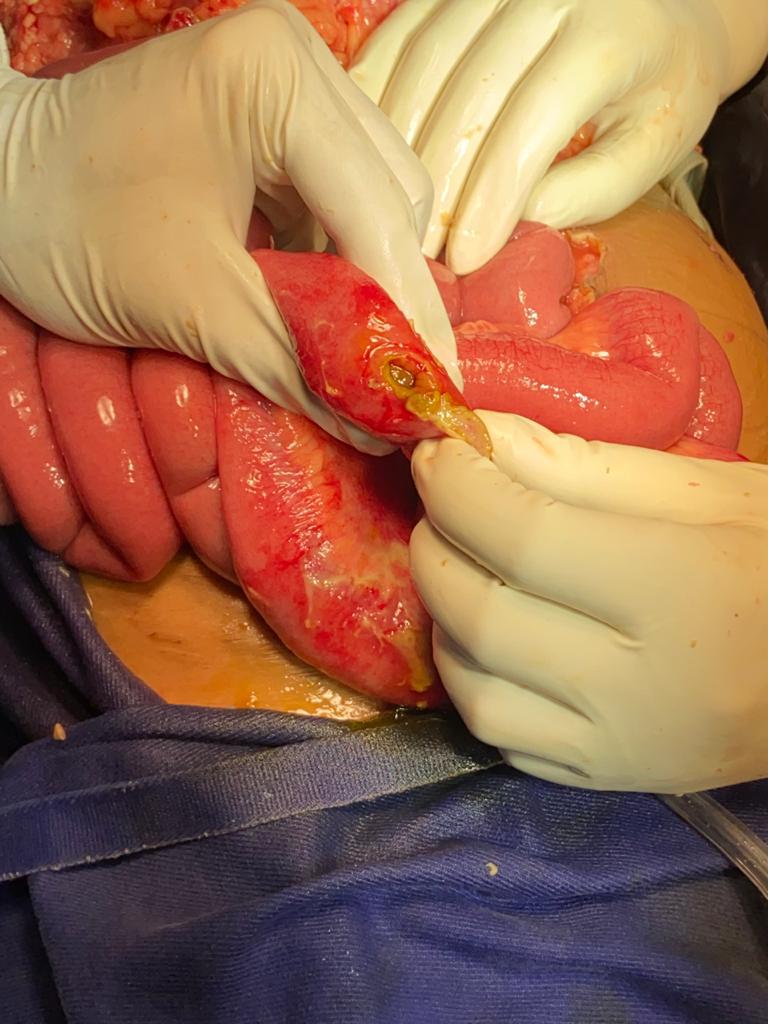
5.7.21 The abdomen was opened through midline incision for a full laparotomy and it was found there was a big mass of adherent small gut loops which could not be separated; hence the mass was excised and an end-to-end anastomosis (ileo-ileal) was performed.

This time she recovered very fast and very satisfactorily, passing stool and flatus on 2nd postoperative day, and started with oral intake 4th day onwards. Ready to be discharged home today (14.7.21).
Cervical polyp
Posted on: June 13, 2021
13.6.21
A big cervical polyp was removed along with the TAH and BLSOP (Dr Shalley’s case).

28.3.21
An obese man, Tejinder Singh (c/o Balwinder OTA) thought to have inguinal hernia gave great difficulties at inguinal exploration, the fluid of hydrocele present in the cord itself gave the appearance of a big direct or possibly sliding inguinal hernia and the cord dissection took a very long time. Eventually a small indirect sac was found but some more cord dissection led to a lot of fluid appearing in the field. It was all sucked out and the mesh repair performed. More than two months later the patient presented with a large hydrocele refilling and venereal warts on his prepuce and glans. So, after treatment of his genital warts, hydrocelectomy with epididymoorchiectomy had to be done on 23.6.21.
2.4.21
A monopolar diathermy small bowel injury during laparoscopic tubectomy (by gynae) about 5 days back resulted in peritonitis and gas under the diaphragm on x-rays. At urgent laparotomy by the assistant professor (Dr Abhishek), a thorough wash of the peritoneal cavity was done and the perforation exteriorized.
3.6.21
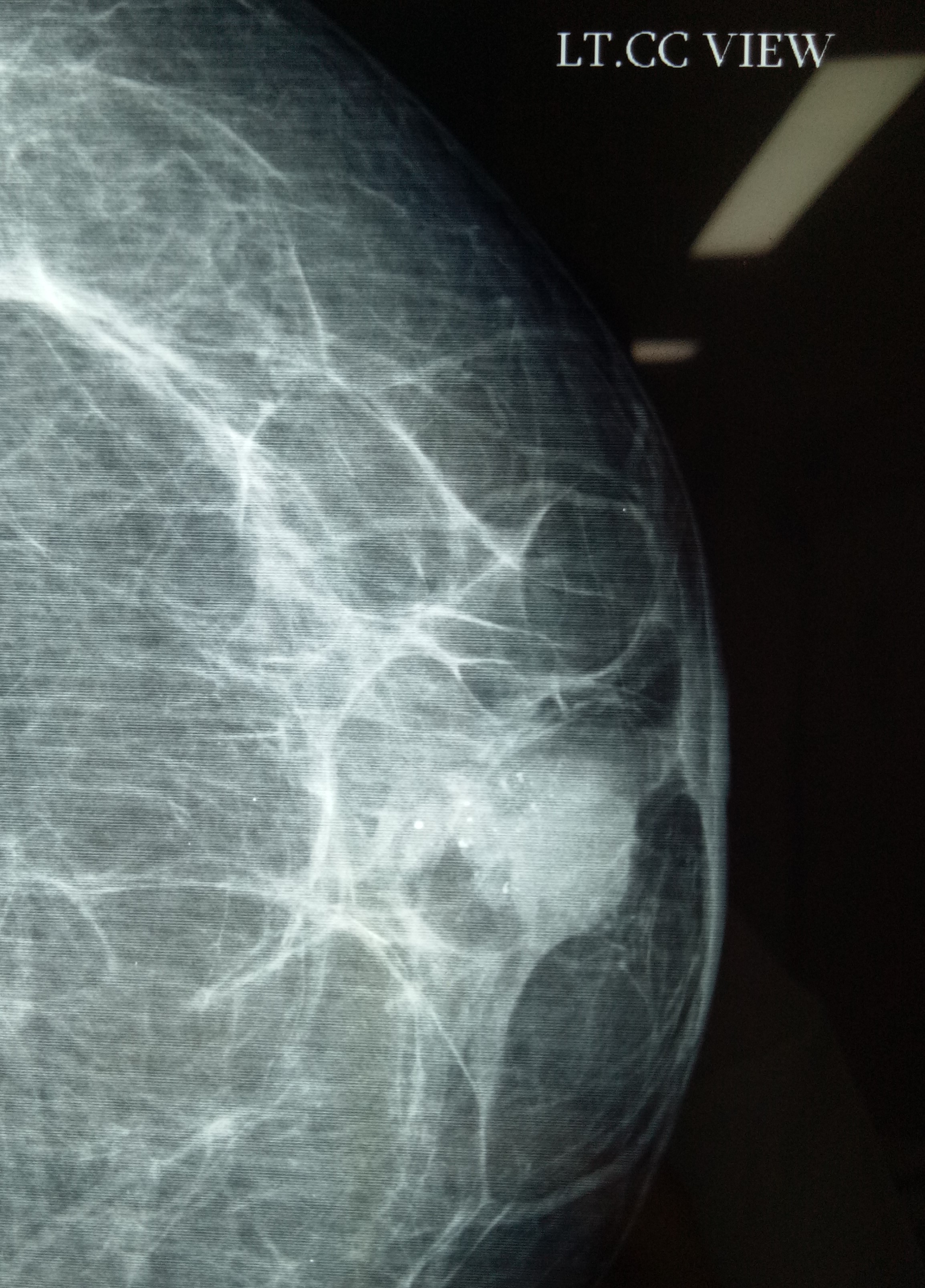
MRM for lobular carcinoma of breast (Dr Jagga’s case). Small tumor (less than 4 cm) and not expected to have metastases in axillary lymph nodes (which were not palpable) actually turned out to have a mass of several enlarged lymph nodes during axillary exploration.

18.10.20
An interesting encounter with gall stone disease: A 55 years old female (mother of Neetu, worker in OT of Shalley hospital), obese and diabetic and hypertensive was known to be carrying gall stones for many years. She landed up in septic shock (cholangitis) and severe pancreatitis and jaundice. Was luckily resuscitated and survived. An urgent ERCP (dr Atul) and stone extraction and stenting the bile duct followed. She reported passing her stent per rectum about 3 weeks later. Luckily the subsequent lap chole was not very difficult.
28.11.20
Another lesson in lap chole: an apparently easy lap chole (as per dr Jagga’s opinion) in a 55 years old female turned out to one of the most difficult and took more than 3 hours. First of all, the duodenum was adherent high up to the fundus which was very thick walled. This was carefully dissected safely. Next the cystic duct was thick walled and friable and the vicryl ligature cut through. Luckily the stump then could be clipped with two large clips. Thirdly, when beginning the dissection of the gall bladder it appeared as if the infundibulum was actually below where the cystic duct had been clipped. But by careful further dissection a safe plane behind the gall bladder could be created and what looked like the infundibulum was actually an large cystic lymph node (fallacy of perception).
Open CBDE
Posted on: June 13, 2021
27.7.20
Open cholecystectomy and CBD exploration after 4 failed attempts to clear the duct endoscopically, including two in the PGI.
5.9.20
An unusual encounter with a a femoral hernia in 60 years old male (s/o old retired laundry incharge RHP) who had been diagnosed as irreducible inguinal hernia. It actually turned out be not inguinal but femoral and mesh repair could be done through the inguinal incision itself.
7.10.20
A lap chole in a 45 years old male had to be converted due the the thick and big omental cake inseparably adherent to the thick walled gall bladder and duodenum. Even at open surgery, the procedure turned out to be very difficult due to dense adhesions around the Calot’s triangle.
16.10.20
Huge bilateral sliding inguinal hernias in an elderly gentleman (related to dr KD Singh, ex-principal GMC Patiala) who was carrying these hernias for more than 10 years. Took more than 2 hours for the bilateral mesh repair.
Locating an undescended testis laparoscopically, and a fallacy of perception in lap chole
Posted on: June 13, 2021
11.6.20
Called by dr Vikram while operating for right undescended testis in a 25 years old male but unable to find the testis in the inguinal canal.
The testis was easily located in the abdomen laparoscopically and removed laparoscopically through the inguinal incision already made.
22.7.20
An apparently easy lap chole became difficult due to two unforeseen problems – firstly due to the gall bladder being intrahepatic and secondly due to the small stones stuck in the fibrosed neck above which the gall bladder apparently narrowed down to the calibre of the cystic duct.
The first problem (the intrahepatic gall bladder) led to difficult and bloody dissection of the cystic artery which was eventually controlled. The second problem caused a fallacy of perception giving the appearance of the cystic duct to the infundibulum of the gall bladder. The dissection here too became very difficult and led to a tear in what was taken to be the cystic duct. A reappraisal of the thought process led to some dissection very low down and deep down to eventually find the real cystic duct just below the fibrosed neck of gall bladder with small impacted stones in it.
Just another example of visual fallacy of perception that so often causes trouble in lap chole.
Ileo-ileal intussusception
Posted on: May 15, 2020
15.5.20
A 50 years old male with a history of recurrent abdominal pain was diagnosed with gallstones and multiple lipomas in the terminal ileum on CT scan. After lap chole by Dr Vikram, a lower limited laparotomy was performed to discover an ileoileal intussusception and the segment of terminal ileum was excised. Cut specimen showed multiple benign looking masses.



16.3.20
A 12 years old male child was operated in the left groin on the suspected diagnosis of a hematoma (history of trauma and diagnosed on ultrasound). Actually turned out to have a nice encysted hydrocele of the cord which was excised, after disconnecting its connection with the processus vaginalis. Dr Jagbir’s case.
Neurofibroma misdiagnosed as popliteal cyst; A Spigelian hernia and a multicentric lobular carcinoma of the breast
Posted on: May 15, 2020
15.11.19
A 50 years old male presumably with a popliteal cyst in the left popliteal fossa turned out to have a neurofibroma actually.

A big lipoma of the thigh resected at GSMCH in a 55 years old man.
3.12.20
A spigelian hernia in the left lower abdomen just above the previously repaired inguinal hernia, repaired with mesh – the patient a 70 years old man Narinderpal singh. Previously operated also for similar right sided spigelian hernia by me some 7 or 8 years back, that side also having had a previous inguinal hernia repaired more than 20 years back. Thus this unfortunate man had 4 lower abdominal and inguinal hernias all of which had to be repaired.
27.1.20
An MRM of the left breast was performed for multicentric lobular carcinoma in a 45 years old female. Dr Jagbir’s case.
Prolonged ileus, pancreatitis and bile leak successively after LC, Cystogastrostomy and cholecystectomy
Posted on: October 27, 2019
17.8.19
A routine lap chole in a 55 years old female turned out to be unexpedtedly difficult, resulting in considerable bleeding from the liver bed. This was controlled with cautery and pressure with gauze, and several pieces of gelfoam were later pressed into the area. Discharged the next day, had to be readmitted on 19.8.19 with abdominal distension. Treated as ileus with IV fluids and recovered by 21.8.19.
2.9.19
Another lap chole case had to be readmitted on 4th PO day for severe abdominal pain, possibly pancreatitis. resolved with conservative treatment in 2 days.
23.9.19
Another lap chole landing up in trouble. A young 30 year old male underwent a very difficult lap chole due to the frozen Calot’s triangle and a very thick-walled gall bladder. Postoperatively had a bile leak which was 200 cc on the first postoperative day and then continued to decrease in amount gradually drying up in 18 days. MRCP reported a small collection and a ? kink and narrowing at the site of cystic duct-CBD junction. the radiologist’s reported this as a cystic duct blow-out!

24.9.19
Cystogastrostomy and cholecystectomy in a 65 years old female who was admitted more than 2 months back in ICU for severe pancreatitis. Had developed a big pseudocyst which continued to persist and cause pressure symptoms.
 A lot of necrotic debris was also removed from the depth of the pseudocyst cavity.
A lot of necrotic debris was also removed from the depth of the pseudocyst cavity.
9.10.19
An attempted lap chole in an 85 years old man (Dr NP Singh’s case) was abandoned, due to dense adhesions and the liver being very hard and cirrhotic with innumerable nodules on its surface.
