Screws removed from my NOF fracture, and a problem with open ureterolithotomy
Posted on: February 6, 2022
16.1.2022
An open ureterolithotomy was performed for a right ureteric stone but it appeared a fragment of the stone migrated up into the dilated system. The ureter was stented and the wound closed. The patient recovered uneventfully but will need endoscopic urological assistance in removing the stent at which time the migrated stone fragment may also be removed.
17.1 2022
My NOF (neck of femur) screws that had been placed there in 2016 for the fracture but were now causing pain were removed under spinal anesthesia.

11.12.2021
Medical college Patiala (GOMCO) batch of our class reunion held in mandi gobindgarh desh bhagat university. Enjoyed.
28.12.2021
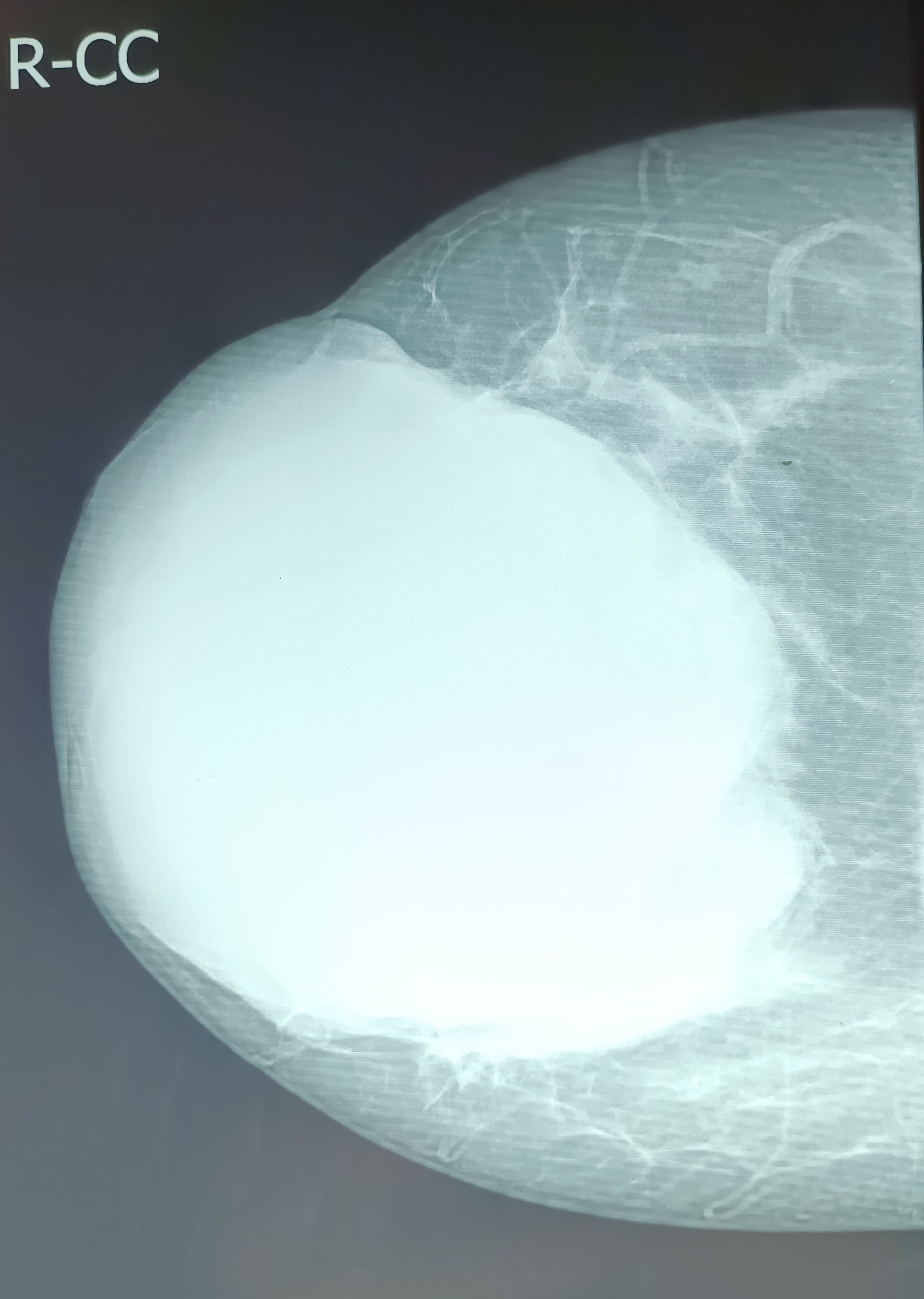
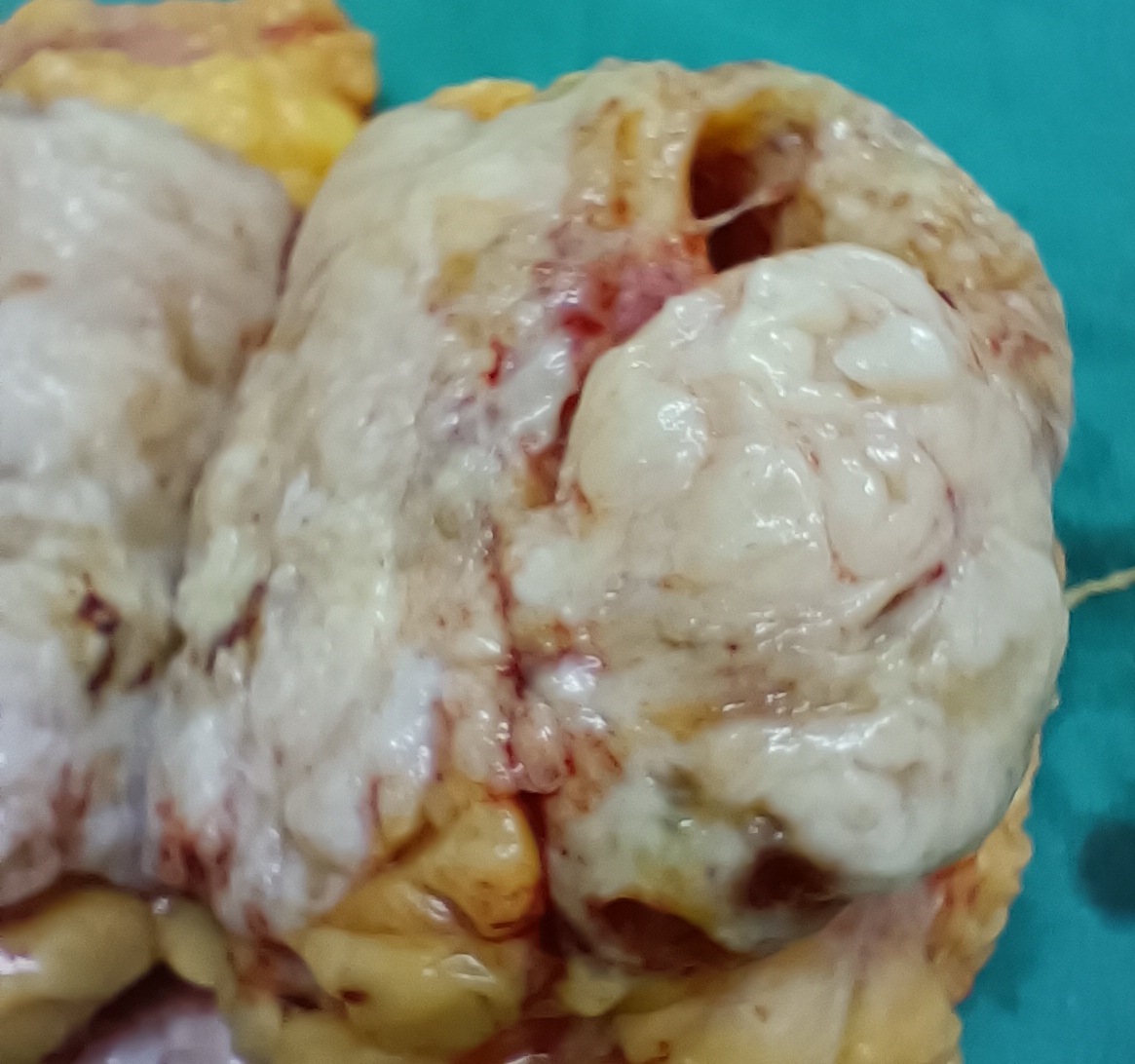
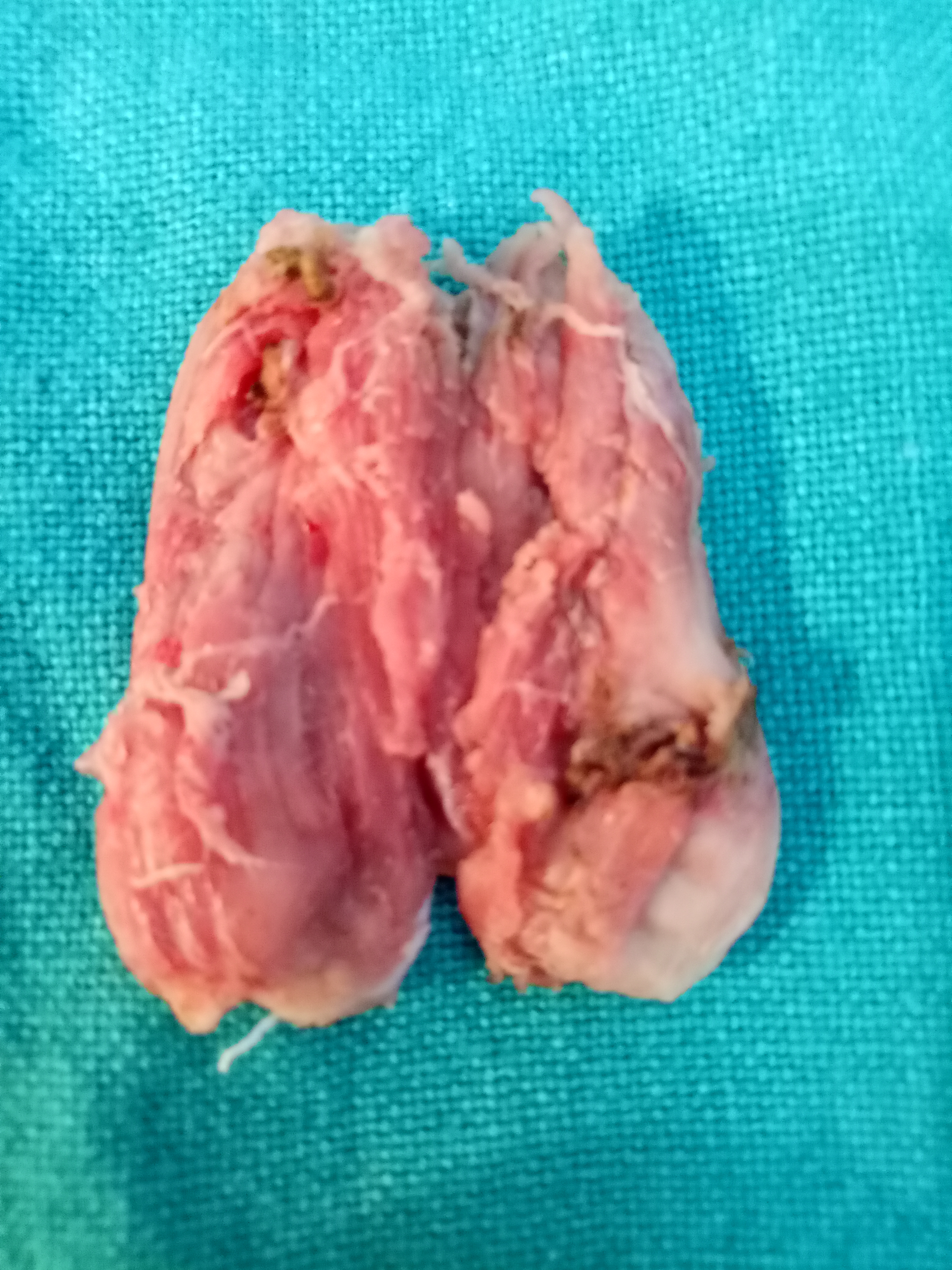
A big phyllodes tumor of the right breast removed at a simple total mastectomy (Dr Jagga’s case).



27.11.21
An appendicectomy in a 45 years old man was found to be difficult, the appendix being high up and retrocecal, necessitating the enlarged muscle-cutting incision. A big fecolith was palpable in the appendix and its tip had begun to be gangrenous.


29.11.21
A large sebaceous cyst on the back of an employee of Shalley hospital was found to be highly inflamed, so was put on antibiotics for the present.

Cysticercosis cellulosae chronic abscess in the forearm muscles, and my facial abrasion
Posted on: November 4, 2021
A chronic swelling in the right forearm of a 7 years old child was was excised from within the forearm flexor muscles. Cut section revealed thick walls and small lumen, possibly cysticercosis cellulosae.


A facial abrasion, sustained from a fall from the bicycle, healed well in five days.





27.10.21
A lap chole presumed to be easy in a 45 years old female took quite a while to clear the anatomy of the cystic pedicle. Just under the small Hartmann’s pouch, a peritoneal band looked exactly like the cystic duct. And above it what was actually the cystic duct was therefore taken to be the cystic artery. But in view of dense adhesions around it, dissection was stopped here, and started again from the middle of the gallbladder downwards, and this cleared the confusion. The cystic artery was later found on the right side.
13.10.21
A 65 years old lady from Rajpura had lumpectomy done at Rajpura (biopsy not done), and then again (possibly wide local excision, biopsy phyllodes) at Patiala, underwent MRM and AC (small shotty lymph nodes palpable in axilla).



17.8.21
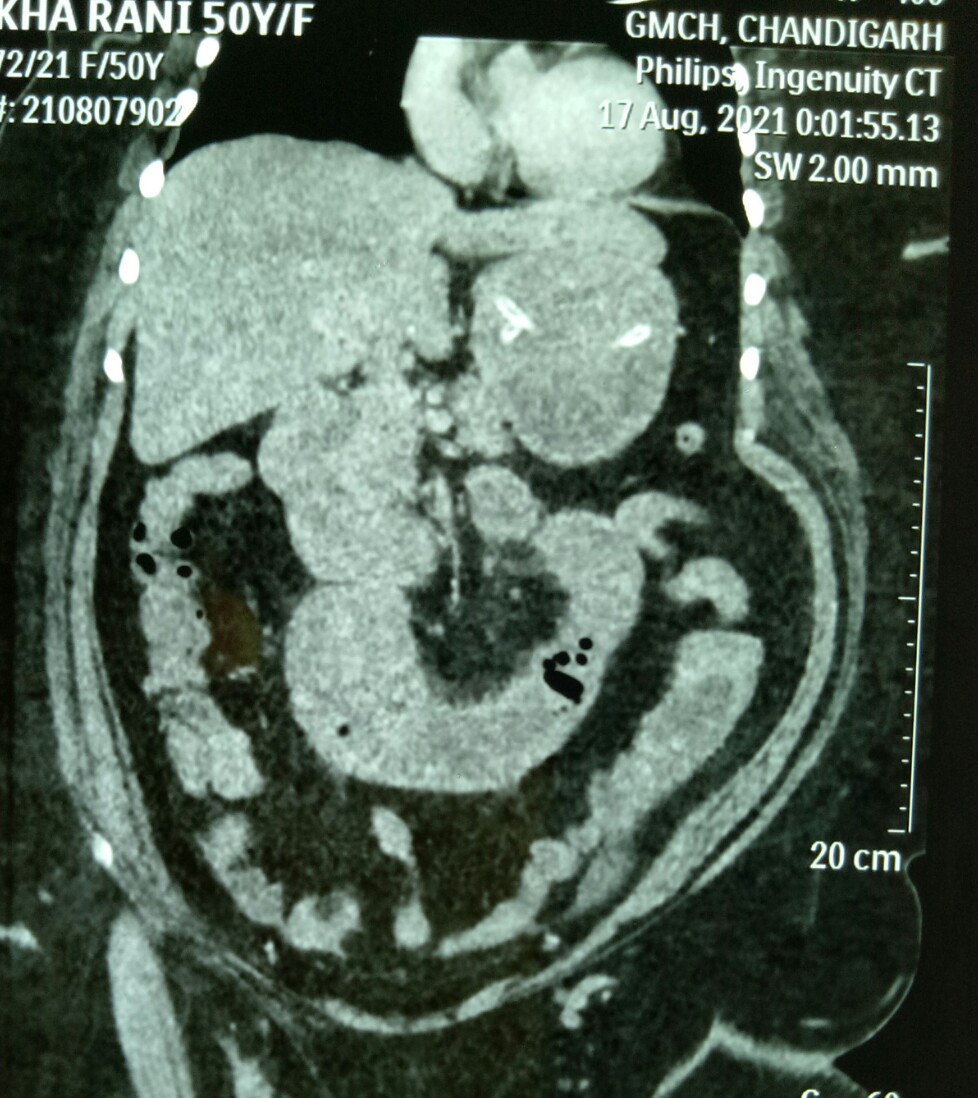
Rekha Rani, 45 years old female, presented with the diagnosis of gastric outlet obstruction (GOO) (on ultrasound!) at Shalley hospital, and was referred to Chandigarh GMCH. There a CT scan showed high SBO (in jejunum), pneumobilia and a stone impacted in proximal jejunum causing the obstruction (Rigler’s triad). At laparotomy, an enterotomy was done to remove the stone and enterotomy closed.

Piecemeal removal of thickwalled difficult gallbladders offers many advantages
Posted on: August 28, 2021
25.7.21
A thick-walled gallbladder (with empyema and some gangrene in the fundus) removed in several pieces through the epigastric port without dilating or enlarging the port;

this has been the practice now for many years with me as it offers so many advantages:
- Grasping the gallbladder which has grossly thick and tough walls and which is often very big and tense (sometimes empyema or mucocele) is impossible; so opening the fundus first of all helps in suctioning the mucus or pus and decreasing the size of the gall bladder. The large stones are also removed from within and the empty gall bladder is washed clean. Now the grasper can easily hold the left or the right flap.
- The dissection if easy in the Calot’s area can now be attempted and completed if it is easy. If not, stop (time out);
- Most often in these cases the infundibulum too is grossly thick and can’t be held with the grasper; so, the incision from the fundus is extended down to the infundibulum and the anatomy re-evaluated after the grasper can hold the fundus flap on the lateral or medial side.
- Since the gallbladder is now of manageable size and can be held comfortably and the posterior wall of the gallbladder viewed closely with the camera zoomed in, dissection can begin above the Rouviere’s sulcus level on the medial side high up near the middle of the body of the gallbladder with a hook separating the peritoneum if possible and then if easy, the Calot’s triangle can be dissected as usual. If not easy, again stop (time out).
- More often than not, however, the peritoneum is fused with the thick walls of the gallbladder and no plane of dissection is safely available.
- In such cases, starting again high up, a plane can be created with a hook through the thickened walls of the gall bladder and then with a suction cannula and a piece of gauze as dissecting tools one can often go safely behind the posterior wall or behind the mucosa of the posterior wall to emerge on the lateral side.
- This plane of dissection (mostly submucosal, under the mucosa or through the thick wall) is then extended down similarly with gauze and hydrodissection, occasionally assisted by the hook to cut away a tough adhesion, always under clear and close vision of the camera, down to the infundibulum or the neck of gallbladder whichever appears to be the narrowest part which is then simply ligated with no 1 vicryl using extracorporeal knot. Before doing this one must again confirm through the opened up gallbladder that no stone is left behind in the gallbladder.
- The GB is simply divided just above the knot and removed, but the posterior wall of the gallbladder is left behind, the mucosa to be cauterized just before closure.
- The 2 big flaps of the gallbladder still be need to be divided into more vertical strips to make it easier to remove those strips through the epigastric port one by one; thus ensuring:
- The procedure remains minimal access still, and
- The troublesome problems of gas leak and the heightened risk of incisional hernia through the dilated/enlarged port are avoided.
Moral and ethical issues in surgery – a ruptured tubal pregnancy; tubectomy or the other side – yes or no?
Posted on: August 5, 2021
4.8.21
A ruptured ectopic right tubal pregnancy wit hemoperitoneum in a 35 years old female was operated urgently due to severe pain in the RLQ; the US showing ectopic tubal pregnancy. A salpingectomy of the involved tube removing the products of conception in the tube was done along with peritoneal lavage. The lady repeatedly was talking under spinal anesthesia for tubectomy on the other side too. I asked the attending gynecologist dr Neena Sachdeva and she said the husband did not want it. So we did not do it. The next day during another surgery (LSCS), Dr Neena reported that the lady had married her present husband without telling him that she had had an earlier marriage and that she had 2 more children from that and so she did not want any more children and wanted a tubectomy on the other side too. She said it was right that we did didnt do the other tubectomy otherwise legal issues might arise later!
Branchial cyst
Posted on: July 20, 2021
8.7.21
A typical cystic swelling in lower left neck anterior to sternocleidomastoid in a 10 years old boy, typical of congenital branchial cleft cyst. Cytology supported the diagnosis (cholesterol crystals, squamous cells), but ultrasound suggested lipoma! Easily excised through a transverse incision. No associated sinus or fistula track.

