20.2.09
Went to Gian Sagar Medical College, saw the chairman (mr Bhangoo) and vice-chairman (dr Sukhwinder singh), discussed with them about joining them and decided to do the same full time.
21.2.09
Gave joining report as Professor to dr Kamaljit singh CEO.
23.2.09
Went to GSMC, saw dr Sekhon (the principal) there, and changed the plan of working there to ‘retainer plan’. (retained for occasional visits).
27.2.09
Amputation b/k, diabetic 60M, infected and gangrenous leg. Wound kept open. Still got infected again later and the skin sloughed. Had to be refashioned after cutting further a bit of the femur on 15/4/09.
28.2.09
Laparoscopic salpingectomy and removal of a chronic right tubal ectopic pregnancy.
3.3.09
A nightmarish lap chole. 50M with previous history of some procedure in RUQ (?subphrenic abscess drainage or cholecystostomy?). Dense mass in Calot’s triangle. After dissecting out dense adhesions with pylorus and duodenum, neck of gall bladder ligated and transfixed. POD1 reportedly leaked bile through drain, thereafter developed a big septic abscess around the drain site, opened and debrided under anaesthesia (necrotising fascitis ); developed frank faecal fistula later and was referred to DMC Ldh.
10.3.09
my own practice, first case: RIH 63M, easy Lichtenstein.
13.3.09 and 15.3.09
Two successive ‘humping right hepatic arteries’ at lap choles, one too densely adherent to cystic duct, so the gall bladder ligated at the neck.
16.3.09
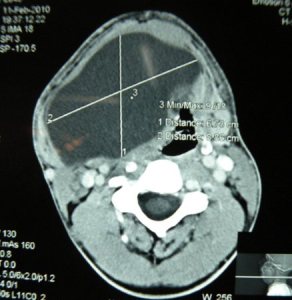
Unexpected postop course for an open prostatectomy 65M. 9th post operative day, had a grand mal seizure. CT showed a big mass (meningioma?). referred for neurosurgery.
17.3.09
Tried unsuccessfully a retroperitoneal laparoscopic ureterolithotomy 50M. Space difficult to maintain due to obesity. Converted to open ureterolithotomy, a big stone in lower ureter removed.
25.3.09
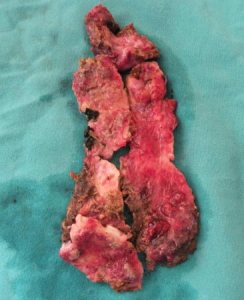
Neglected long-standing hamartoma of face 25M. Development of vision had suffered. Difficult excision of the firm and fibrotic mass almost all over the right half of the face.
26.3.09
Ill-advised and ill-fated laparotomy. 45M with h/o 4 days abdominal distension and pain. USG- collection intraperitoneal. Paracentesis – dark blood. Opened with provisional diagnosis of gangrene gut, but had actually haemoperitoneum. Nearly 2 litres of blood. Fresh bleeding coming from metastatic liver nodules, not picked up by the scan. Spurting vessels from the hard nodules near the porta, could not be controlled. Packed and referred to PGI, but died there the same day. Never had such a shocking experience earlier.
27.3.09
MS2: Occipital menigocele repaired. 1 month old female child.
28.3.09
Supposedly a thyroglossal cyst in midline 11 months old female child, turned out to be a mucous cyst only in the submandibular region (?from minor salivary glands).
A very long intersphincteric fistula-in-ano; reucurred. 50 M from Kheri, obese. All track excised. took 2 months to heal.
29.3.09
A similar high intersphincteric fistula-in-ano excised; again recurred and 50M.
30.3.09
lLaparoscopic salpingotomy for an unruptured ectopic pregnancy. Tube repaired with 4/0 vicryl.
4.4.09
Lap appy became ovarian cystectomy when the diagnosis changed to ruptured ovarian cyst on laparoscopy. 25F.
7.4.09
3 difficult cases:
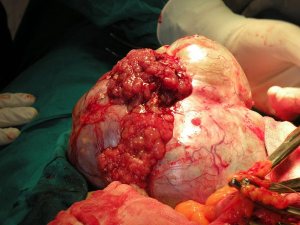
Left nephrectomy for renal cell carcinoma. Obese 54 M, father of an MD psychiatry doctor from Ludhiana. A single episode of haematuria. CT showed 5 cm tumour left kidney upper pole. Anterior transperitoneal approach, the whole thing mobilised along with spleen and tail of pancreas. Spleen preserved, but some of tail of pancreas, being adherent with the tumour, excised along with the specimen. This tail was closed with silk sutures.
Lap chole 50 F, difficult due to thick-walled gall bladder, empyema and gangrene of wall of gall bladder.
Hydatid cyst of segment 8 of liver, very high under the diaphragm and adherent to it. Very difficult approach and procedure. All membranes removed after injection of hypertonic saline. Cavity obliterated with capitonage and at the end with a plug of omentum. Had fever postoperatively from POD1 and persisted for nearly a month, due to atelctasis and a patch of pneumonitis right lower lung zone.
10.4.09
Converted lap chole after finding very dense inseparable omental adhesions with gall bladder all over down to the neck, producing a big hard mass. 25 years young male with previous ERCP and ES for CBD stones, stones removed and CBD stented. At open operation, gall bladder opened, stones removed and a partial cholecystectomy done, ligating the neck from within. Finding a central dark patch ( a possible perforation of pyloroduodenal area) on the surface of the centre of the thick inflammatory mass which had been separated from the gall bladder, decided to open it and freshen it up and close it again, but when it was cut with scissors with this intent, the mucosa still escaped the scissors, so was closed with seromuscular sutures. Another new experience.
17.4.09
Bilateral inguinal direct herniae repaired with mesh. Dr Sat Pal from Mansa.
A high interphincteric fistula again. 9 cm long track on MRI. 50 M again with recurrence. The track went rght upto the ischial tuberosity. Postop had foot drop, related to the lithotomy position, recovered over 2 months.
21.4.09
A perianal abscess, extensive, going almost all around the anal opening except the left lateral 1/3rd of it. 25M who turned out to be diabetic and the abscess unexpectedly bad with extensive necrotic areas in it. All thoroughly debrided.
22.4.09
MS6: PUH repair. 62M.
23.4.09
An abdominal hysterectomy getting into unexpected problems. A simple easy and satisfactory TAH done on a 60 F. Next day reported to be in anuria with passage of scanty blood-stained urine and very low BP. ? ligated ureters, ruled out on ureteroscopy and contrast study. Explored on seeing blood oozind out of the wound and suspicion of ?intraperitoneal haemorrhage. Found none, except ooze from all over, ?DIC. Then it transpired that she had a blood transfusion yesterday just before the operation. Mismatched?
30.4.09
Excision of a left thigh swelling. Cystic hygroma. 10 year old male child. MRI suggested a hamartoma.
4.5.09

Intussusception, irreducible. REEA 11 month old child.