Archive for the ‘Uncategorized’ Category
5.2.10
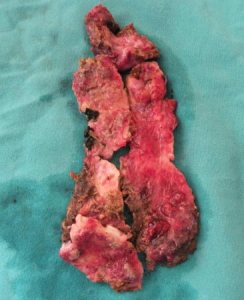
Haemangioma of neck. 45F with long standing swelling right neck, compressible but not expansile. Excised under GA.
Lap chole for huge empyema, 50 M. Aspirated before operation under US to emptiness. Later at operation, the huge thick walled gall bladder removed in 5 pieces.
6.2.10
TLH
12.2.10
A difficult lap chole for empyema. 45 M with empyema gall bladder, wanted early operation. Big stone from within the gall bladder removed after fragmentation.
16.2.10
TEP right indirect inguinal hernia. 25 M. the sac divided and endlooped. Poor light and leaking trocars!.
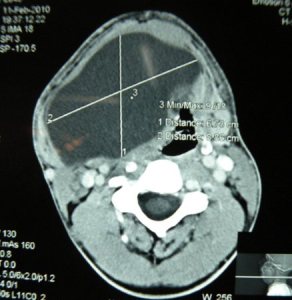
A huge swelling right neck in 25 M, pressing on trachea and shifting it to other side. bulging in floor of mouth. Excised under GA. contents like dermoid.



18,19,20 february
attended the annual conference of IAGES at Delhi..
21.2.10
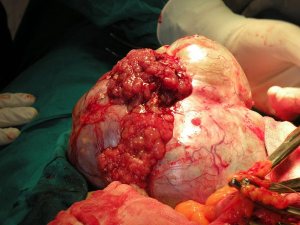
A huge fungated ovarian tumour, malignant, 45F. TAH bSOP and omentectomy. Clinically presumed to be benign in an otherwise very fit looking patient.


15.12.09
La chole: ward worker, obese hypertensive lady 55 yr old.
Lap chole: 65 F admitted last week with gallstone pancreatitis which had resolved by now. Readmitted 25.12.09 with severe abdominal pain.
18.12.09
Lap repair of paraumbilical hernia.
Lap varicocelectomy 20 M.
19.12.09
Irreducible direct left inguinal hernia which had sigmoid colon nearly strangulated. 60M. Cord divided and mesh repair done.
20.12.09
(winter vacation 20.12.09 to 2.1.10).
TAHbSOP with sacrocolpopexy and mesh fixation of rectum to sacrum too for rectal prolapse. 65F from the hills with uterine and rectal prolpase. Had postop SBO due to adhesions for which laparotomy and adhesiolysis had to be done.
22.12.09
TLH for big fibroids made handling of uterus difficult. Took nearly 3 hours.
23.12.09
lap appy 25M, easy.
TEP for direct left inguinal hernia. 25M. Neat despite pneumoperitoneum and despited avulsion of inferior vascular pedicle which was simply coagulated and divided.
24.12.09
Laparotomy for suspected appendicitis which turned out to be biliary peritonitis in a 6 years old male child. The cause of bile leak traced to CBD the anterior wall of which had necrosed (cause??)and oozing bile. Repaired with cystic duct flap over a T rube.
28.12.09
TLH for huge uterus due to huge fibroids reaching upto above the umbilicus. Took nearly 5 hours. The uterus had to be cut into 4 pieces to be removed per vagina (morcellator not available).
Joining govt service again, and some surgeries (including an adult intussuception and a hymenectomy).
Posted on: June 21, 2009
24.5.09
Acute gangrenous appendix removed laparoscopically urgently at 10 pm (c/o dr parminder from barnala). Young 12 male child.
27.5.09
A twisted ovarian cyst clinically and radiologically diagnosed, excised laparoscopically. 15 years old female with severe unremitting pain for 5 days (c/o milkman). However ovary was seen separate from the mass, and therefore it was surmised the mass was arising from the tube.
1.6.09
12 male child with a preoperative diagnosis of varicocele, causing pain. At inguinal exploration, had an indirect hernial sac which was the most likely cause of pain. Herniotomy and ligation of varicocele done.
4.6.09
Joined GMC patiala again as professor after the notice of premature retirement given in february was allowed to be withdrawn by the government.
5.6.09
Laparotomy for intestinal obstruction of some days standing. Remained admitted with medicine department with lots of investigations – including CT and BMFT but not operated. At operation, had intussusception – ileoileal. REEA done. A tumour within the lumen seen on cut section of the specimen.
7.6.09
day case lap chole 5. postop fever upto 101, settled in evening.
11.6.09
TLH satisfactory and complete.
12.6.09
TEP repair of left inguinal hernia. Very satisfactory and clean at last. 50 M with small direct hernia.
14.6.09
TLH satisfactory. Obese female 45 y o with posterior fundal fibroid.18.6.09
18.6.09
Hymenectomy for imperforate hymen. 17 F with big haematocolpos and haematometra.
21.6.09
a possible CBD injury:
an easy looking lap chole became difficult. 35F. while creating the posterior window and dividing the peritoneum posteriorly, bile leak noticed, presumable due to accessory duct. The patient was later found to have a RHD injury. Sad.
Tryst with GSMC, and starting my own surgery, a hamartoma, a cystic hygroma, an intussusception etc
Posted on: May 7, 2009
20.2.09
Went to Gian Sagar Medical College, saw the chairman (mr Bhangoo) and vice-chairman (dr Sukhwinder singh), discussed with them about joining them and decided to do the same full time.
21.2.09
Gave joining report as Professor to dr Kamaljit singh CEO.
23.2.09
Went to GSMC, saw dr Sekhon (the principal) there, and changed the plan of working there to ‘retainer plan’. (retained for occasional visits).
27.2.09
Amputation b/k, diabetic 60M, infected and gangrenous leg. Wound kept open. Still got infected again later and the skin sloughed. Had to be refashioned after cutting further a bit of the femur on 15/4/09.
28.2.09
Laparoscopic salpingectomy and removal of a chronic right tubal ectopic pregnancy.
3.3.09
A nightmarish lap chole. 50M with previous history of some procedure in RUQ (?subphrenic abscess drainage or cholecystostomy?). Dense mass in Calot’s triangle. After dissecting out dense adhesions with pylorus and duodenum, neck of gall bladder ligated and transfixed. POD1 reportedly leaked bile through drain, thereafter developed a big septic abscess around the drain site, opened and debrided under anaesthesia (necrotising fascitis ); developed frank faecal fistula later and was referred to DMC Ldh.
10.3.09
my own practice, first case: RIH 63M, easy Lichtenstein.
13.3.09 and 15.3.09
Two successive ‘humping right hepatic arteries’ at lap choles, one too densely adherent to cystic duct, so the gall bladder ligated at the neck.
16.3.09
Unexpected postop course for an open prostatectomy 65M. 9th post operative day, had a grand mal seizure. CT showed a big mass (meningioma?). referred for neurosurgery.
17.3.09
Tried unsuccessfully a retroperitoneal laparoscopic ureterolithotomy 50M. Space difficult to maintain due to obesity. Converted to open ureterolithotomy, a big stone in lower ureter removed.
25.3.09
Neglected long-standing hamartoma of face 25M. Development of vision had suffered. Difficult excision of the firm and fibrotic mass almost all over the right half of the face.

26.3.09
Ill-advised and ill-fated laparotomy. 45M with h/o 4 days abdominal distension and pain. USG- collection intraperitoneal. Paracentesis – dark blood. Opened with provisional diagnosis of gangrene gut, but had actually haemoperitoneum. Nearly 2 litres of blood. Fresh bleeding coming from metastatic liver nodules, not picked up by the scan. Spurting vessels from the hard nodules near the porta, could not be controlled. Packed and referred to PGI, but died there the same day. Never had such a shocking experience earlier.
27.3.09
MS2: Occipital menigocele repaired. 1 month old female child.
28.3.09
Supposedly a thyroglossal cyst in midline 11 months old female child, turned out to be a mucous cyst only in the submandibular region (?from minor salivary glands).
A very long intersphincteric fistula-in-ano; reucurred. 50 M from Kheri, obese. All track excised. took 2 months to heal.
29.3.09
A similar high intersphincteric fistula-in-ano excised; again recurred and 50M.
30.3.09
lLaparoscopic salpingotomy for an unruptured ectopic pregnancy. Tube repaired with 4/0 vicryl.
4.4.09
Lap appy became ovarian cystectomy when the diagnosis changed to ruptured ovarian cyst on laparoscopy. 25F.
7.4.09
3 difficult cases:
Left nephrectomy for renal cell carcinoma. Obese 54 M, father of an MD psychiatry doctor from Ludhiana. A single episode of haematuria. CT showed 5 cm tumour left kidney upper pole. Anterior transperitoneal approach, the whole thing mobilised along with spleen and tail of pancreas. Spleen preserved, but some of tail of pancreas, being adherent with the tumour, excised along with the specimen. This tail was closed with silk sutures.
Lap chole 50 F, difficult due to thick-walled gall bladder, empyema and gangrene of wall of gall bladder.
Hydatid cyst of segment 8 of liver, very high under the diaphragm and adherent to it. Very difficult approach and procedure. All membranes removed after injection of hypertonic saline. Cavity obliterated with capitonage and at the end with a plug of omentum. Had fever postoperatively from POD1 and persisted for nearly a month, due to atelctasis and a patch of pneumonitis right lower lung zone.
10.4.09
Converted lap chole after finding very dense inseparable omental adhesions with gall bladder all over down to the neck, producing a big hard mass. 25 years young male with previous ERCP and ES for CBD stones, stones removed and CBD stented. At open operation, gall bladder opened, stones removed and a partial cholecystectomy done, ligating the neck from within. Finding a central dark patch ( a possible perforation of pyloroduodenal area) on the surface of the centre of the thick inflammatory mass which had been separated from the gall bladder, decided to open it and freshen it up and close it again, but when it was cut with scissors with this intent, the mucosa still escaped the scissors, so was closed with seromuscular sutures. Another new experience.
17.4.09
Bilateral inguinal direct herniae repaired with mesh. Dr Sat Pal from Mansa.
A high interphincteric fistula again. 9 cm long track on MRI. 50 M again with recurrence. The track went rght upto the ischial tuberosity. Postop had foot drop, related to the lithotomy position, recovered over 2 months.
21.4.09
A perianal abscess, extensive, going almost all around the anal opening except the left lateral 1/3rd of it. 25M who turned out to be diabetic and the abscess unexpectedly bad with extensive necrotic areas in it. All thoroughly debrided.
22.4.09
MS6: PUH repair. 62M.
23.4.09
An abdominal hysterectomy getting into unexpected problems. A simple easy and satisfactory TAH done on a 60 F. Next day reported to be in anuria with passage of scanty blood-stained urine and very low BP. ? ligated ureters, ruled out on ureteroscopy and contrast study. Explored on seeing blood oozind out of the wound and suspicion of ?intraperitoneal haemorrhage. Found none, except ooze from all over, ?DIC. Then it transpired that she had a blood transfusion yesterday just before the operation. Mismatched?
30.4.09
Excision of a left thigh swelling. Cystic hygroma. 10 year old male child. MRI suggested a hamartoma.
4.5.09
Intussusception, irreducible. REEA 11 month old child.
7.1.09
Wedge excision of cancer lip – 45 M with zarda addiction.

9.1.09
A satisfactory TEP after a long time. Right indirect inguinal hernia.
2.1.09 to 16.1.09 vacation
16.1.09
An easy appearing appendicectomy became a hemicolectomy. A fit young 30 M with presentation like appendicitis. On palpation at surgery, the appendix was found to be densely adherent with a high-lying caecum which also had a palpable mass in it, and the right colon was quite considerably shortened. A few small lymph nodes were also palpable in the mesentery. All this was excised and an ileocolic anastomosis made. Path report later was non-specific inflammation. Nonetheless, the treating physician decided to give a course of ATT.
24 and 25 jan –
Conference in Delhi on ‘complications in laparoscopic surgery’ attended. Nicely organised by delhi chapter of ASI.
1.2.08
a shocker of a news – 5 babies in phototherapy unit of rajendra hospital paediatric department burnt alive.
2.2.09
Principal of medical college (dr JPK shergill) and junior resident on duty suspended.
3.2.09
Strike by juniour doctors association against the suspension.
5.2.09
Suspensions of both the JR and principal withdrawn!.
6.2.09
Information that transfers to Amritsar are being made tommorow led to my decision to resign from service.
7.2.09
Gave my premature retirement notice to Principal’s office and resigned.
8.2.09
Gave departure report to Principal’s office.
9.2.09
Inguinal canal of a 6-year-old male child explored for undescended testis on the right, only to find that one was easily found in the canal and another one coming through the ring from inraabdominal location. Thus both testes coming from same side. Never had seen or heard of such a thing.
7.11.08
25M with bilateral undescended testes, right orichiopexy 3 weeks before now for left orchiopexy. Testis high, intraabdominal; could be brought down only after division of testicular vessels (FowlerStephen).
14.11.08
APR: 50 obese lady presenting with tight stenosis of anus, colostomy done 3 weeks before. CT low rectal tumor involving levators. At operation tumour adherent to pelvis side wall too on right side. Removed incompletely, for later radiochemotherapy.
18.11.08
4 lap choles, one after the other, all difficult.
21.11.08
retention cyst minor salivary glands floor of mouth (small ranula) excised under GA 50F.
Trichobezoar removed from a 16F psychotic. helped in stomach closure.
22.4.08
1. diagnostic laparoscopy: 45M fed up with no diagnosis being made for non-specific abdominal pain. the urologist had diagnosed a small ureteric stone which was allegedly removed (no record available). pain still continuing. At laparoscopy, had adhesions in both iliac fossae with abdominal wall; these were easily divided. Appendicectomy too carried out.
2. a quick, easy and neat lap chole
3. a submuscular lipoma left lower chest wall excised under local anaesthesia 25M
4. an extended right hemicolectomy for big tumor transverse colon. Young 25 M with family history of cancer, neglecting his symptoms for 2 years; now reported with bleeding per rectum and at Hb level of 4G%. had 5 blood transfusions.
ascites small amount present. liver clear. but the tumour was locally adherent with omentum and nearly encroaching upon the greater curve of the stomach. was also adherent with the very first part of jejunum being stuck in the DJ flexure. Palliative resection carried out with ileotransverse anastomosis.

a month’s backlog
Posted on: March 21, 2008
22.2.08
Planned LAVH actually became TLH, as dissection could be continued with simultaneous use of bipolar and monopolar diathermy with a single diathermy machine. enjoyed.
23.2.08
AMCA , AMDAANA meet at Amritsar; attended along with dr Ashok and Dr Bir Singh
25.2.08
Attended purchase committee meeting, along with dr Sharda, in DRME office for purchase of sutures
1.3.08
lap chole in ASR
2.3.08
TLH using, for the first time, the harmonic scalpel. enjoyed.
5.3.08
Interesting case: obese 50M rural. h/o intestinal obstruction for 10 days. On exam, irreducible hernia left inguinal. Explored through inguinal incision first; foul smelling fluid in the hernial sac, sucked out. Loops of small bowel (had reduced) examined to find dusky and dark spots at several places and lot of foul smelling (feculent) fluid in the peritoneal cavity; so needed a full laparotomy. Opened through midline incision. Small bowel decompressed retrogradely thru nasogastric tube and eventually returned to healthy colour. However, further examination showed a small perforation in the caecum and a large patch of gangrene in the caecal wall; local resection of small ileocecal segment and EEA done.
Did well post op although did give some sleepless nights.
8.3.08
2 lap choles in Amritsar
12.3.08
Burch colposuspension. Obese 50F. difficult procedure
17.3.08
meeting in DRME office again for purchase of sutures
18.3.08
Tuberculosis nuisance: Young (20) F with almost completed anti-tubercular therapy (DOTS), presented with intestinal obstruction, not responding to conservative treatment for 5 days. Explored to find disseminated tuberculosis – ascites + tubercles all over serosa + adhesions of small bowel loops + old caseated mesenteric lymph nodes + transverse colon stuck to anterior abdominal wall. The transverse colon got injured in the upper part of the incision. Small bowel freed from bands and adhesions and decompressed. The rent in transverse colon repaired.
FIAGES
Posted on: February 18, 2008
feb 14-17 annual conference of IAGES (held at Jaipur) attended along with 5 others from Patiala – dr jagbir, dr sukhpreet, dr grover (with one of his residents) and dr pawan.
Reached jaipur on 13th and stayed at circuit house there.
On 15th saw some of surginet members – dr sayandev and dr ramana from calcutta, dr alexander shoucair from germany, dr samir johna from US and dr danny rosin from israel.
got fellowship of IAGES on 15th
good workshop and conference held at Mahatma Gandhi medical college.
17.12.2007: 3 lap choles
Lap chole in a 50 years old female from Ghagga. Easy.
Another lap chole in a 50 years old female from medical ward.
Lap chole and lap appy in a 55 years old female with persistent pain of appendicitis for more than a week and a previous history of attack of biliary pancreatitis (c/o pharmacist in store, Charanjit Singh).
TEP for bilateral inguinal hernias in a 50 years old male, apparently direct, but turned out to be both indirect sacs, right bigger than left. Quite satisfactory dissection at last. Took nearly 1.5 hours.
