The anatomy of Rouviere’s sulcus as seen during laparoscopic cholecystectomy
Posted on: May 14, 2017
https://www.ncbi.nlm.nih.gov/pubmed/28281470
The Rouviere’s sulcus can now be defined in three simple terms – a deep sulcus, or a slit or a scar. We recommend that as a first step in laparoscopic cholecystectomy, the surgeon must look for this reference point (whether it is in the form of a scar, or a slit or a real sulcus) which will be the plane of the main bile duct, and thus avoid any dissection below this point in order to eliminate any danger to the bile duct during surgery.
 The Scar
The Scar
 The Slit
The Slit
 The Sulcus (open)
The Sulcus (open)
 The sulcus (closed)
The sulcus (closed)
22.3.17
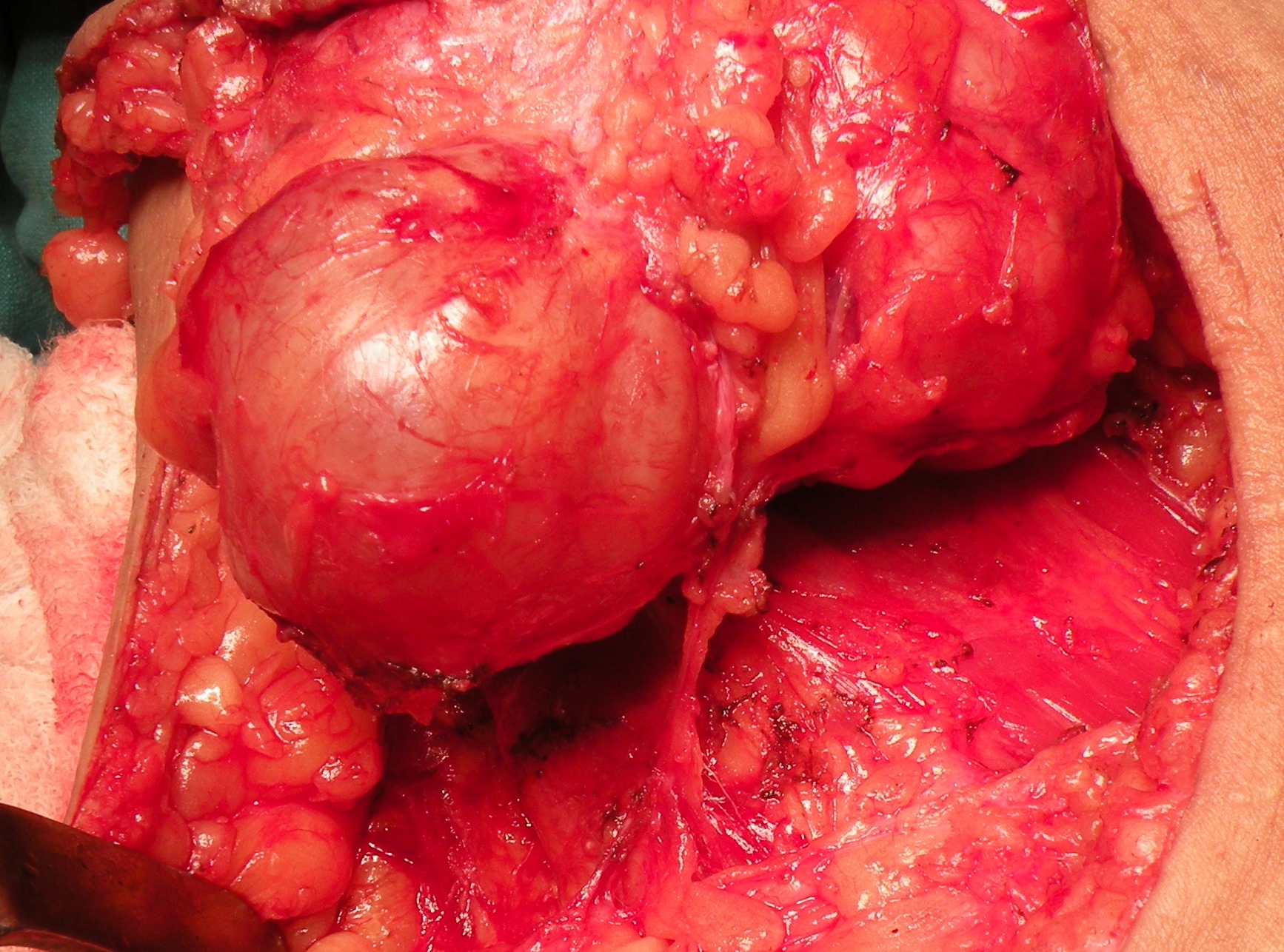
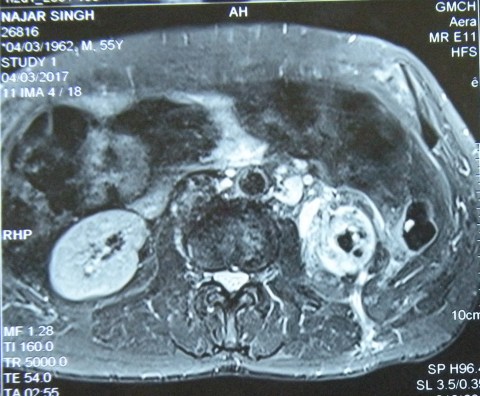
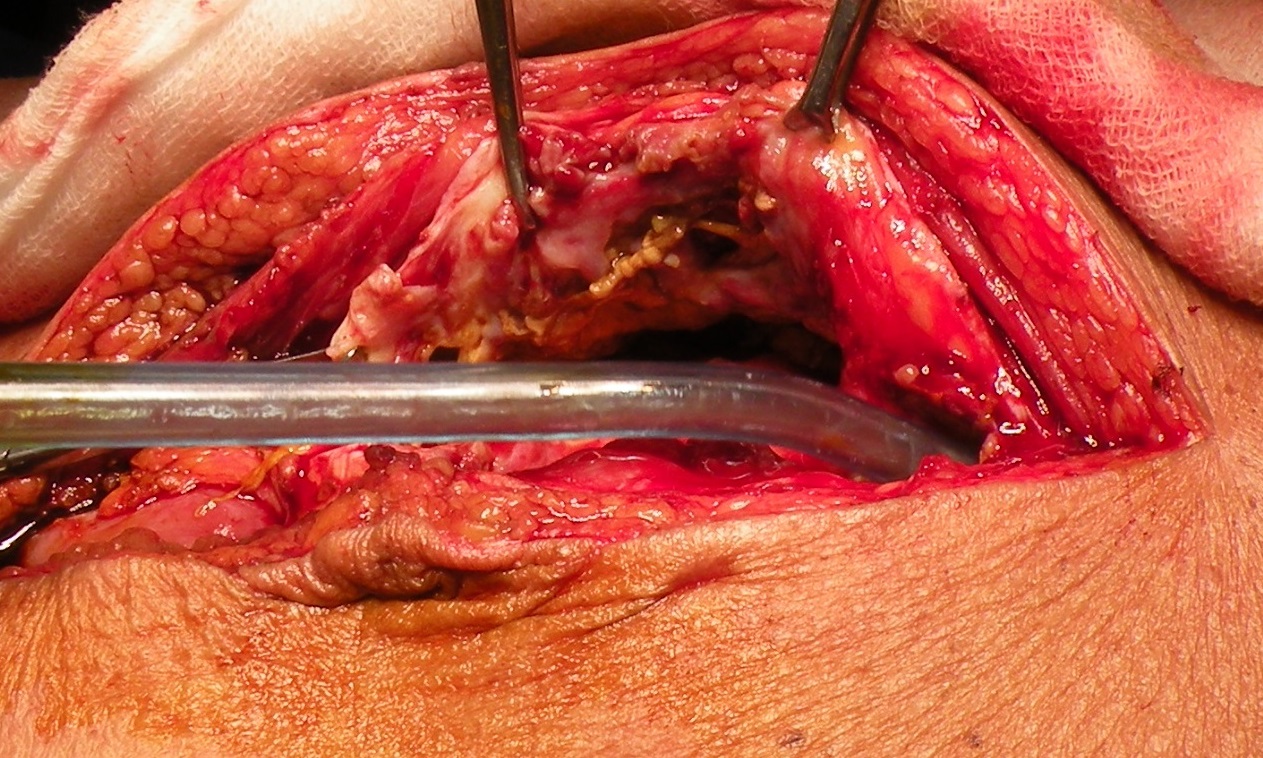
An elderly man (65 years old) presented with a sinus on the back in the loin area, occasionally discharging when the patient passed urine. Investigations revealed a poorly functioning non-salvageable left kidney, and the MRI scan reported xanthogranulomatous pyelonephritis with a nicely outlined fistula through the posterior abdominal wall onto the skin of the back on the left side. A difficult nephrectomy was performed along with excision of the whole fistula tract.


10-13 November, 16
Attended the ICS conference at Guwahati along with dr Sukhpreet, dr Jagga and dr Grover. Also saw dr Bhardwaj there.
21.1.17
Nephrectomy for a huge renal cell cancer with cystic and solid areas, and with a few stones.

25.1.17
A big ovarian cancer with extensive local spread and ascites.- could only be debulked. (c/o dr Dawra, Fatehabad). However, she had a good response to chemotherapy.
22.2.17
Ileocecal resection and resection for multiple strictures of ileum. 58M (c/o SN in OT). Had been having repeated attacks of obstruction for a few months now. An ileocecal mass locally resected. Several strictures in ileum had to be resected with EEA. A quite proximal stricture in jejunum just bypassed with side-to-side anastomosis. Biopsy revealed tuberculosis.
1.3.17
A ruptured mucocele of appendix. 50 years old female , hospital employee. She was admitted with an appendix mass more than two months back and discharged. However, the appendix mass persisted and a few collections developed in the abdomen. These collections were aspirated and an appendiceal mucocele excised at laparotomy, along with excision of a well localised collection in the pelvis.
Disastrous summer vacation this time (1 july to 31 july)
6.7.16 Had a fall at home (tripped while coming out of the bathroom) at around midnight and fractured the neck of right femur. This was fixed with 4 cannulated screws (zimmer) the next day (7.7.16).



The healing time for this fracture is very long (up to 6 months) and the convalescence painfully slow but if one is lucky and remains active and in a positive frame of mind, it does heal in 3 months time. Mine is healing slowly and I am able to walk with a cane or a walker with partial weight bearing on the leg now.
Three and a half months after the fracture, the x-ray picture was considered satisfactory.

Some earlier stories
23.5.16
Binu joined MD course in DMC Ludhiana, having shifted from paediatrics which she had joined already ( and found it too stressful!). Saw Dr Bajwa (HOD) there and had some nice time with him after so many years.
28.5.16
A lesson relearnt. A failed lap appy converted to find a surprise. The thick and short appendix actually hid a small hard growth in the caecum. A right hemicolectomy was done. Cut section showed a stenosing growth.
19-20 june: conducted the PG surgery exam as internal examiner along with other examiners.
29.6.16
Incisional hernia (following TAH through transverse incision!), repaired with mesh the defect through the right side of the incision. Patient an MD anesthesia herself (Dr Parminder from Sangrur CH).
Rectosigmoid cancer
Posted on: May 18, 2016
18.5.16
A huge ovarian cyst of the right ovary (with very little ovarian tissue salvageable) removed laparoscopically (Dr Karnail Singh’s case).
A rectosigmoid cancer resected by assistant professor Dr Walia, and specimen nicely photographed by a final year medical student.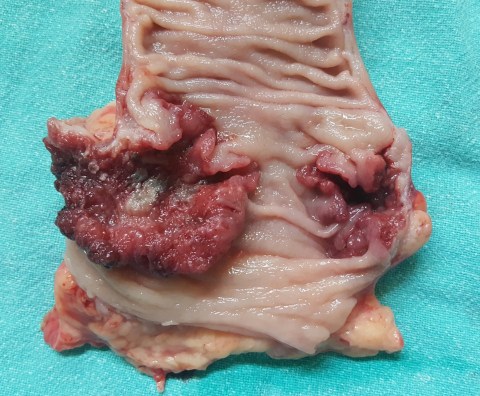
Familial adenomatous polyposis, a huge pseudocyst of pancreas and a choledochal cyst
Posted on: May 17, 2016
5.1.16 to 18.1.16 winter vacation
19.1.16: Following court orders, rechecked theory papers of PG students (who had failed and challenged their failure in court) at BFUHS, Faridkot along with dr Sushil Mittal.
28.1.16 court evidence at Amloh following the issuance of arrest warrants rather than the usual summons for expert witness.
24.2.16
A huge pseudocyst of pancreas in a 25 years old male, proved not to be a cystic neoplasm on investigations, managed by cystojejunostomy Roux-en-Y. The cyst was in the body and tail of pancreas, and parts of its wall had become gangrenous, and had to be excised.

5.3.16
An attempted TEP repair for bilateral inguinal hernias had to be converted to open due to poor relaxation and loss of space.
19.3.16
A choledochal cyst in a 55 years old female, managed by cyst excision and Roux-en-Y hepaticojejunostomy. An anastomotic leak developed and persisted for a long time.
9.4.16
Lap chole in a 62 years old retired doctor (sister of dr Bali, director health and family welfare, Punjab). Thick-walled gallbladder packed with stones. A cholecystohepatic duct appeared high up near the fundus, and was ligated as well as clipped.
12.4.16: Attended court at Dhuri, again following issuance of arrest warrants!

14.5.16
Total proctocolectomy and permanent ileostomy in a 42 years old poor man who had presented with rectal bleeding and severe anaemia, corrected by several blood transfusions. He had a family history of colorectal polyps and also had a duodenal polyp. The distalmost polyps were big and bleeding and possibly malignant and were present in the lower rectum, hence the decision to remove all of distal rectum and anus as well. An abdominoperineal resection and closure of anus were performed after total proctocolectomy was completed.


16.11.15
Multiple big fibroids in a 50 years old lady, causing pain and bleeding. Patient an unmarried jovial lady, and a close friend of Dr Geetanjali. Removed at a total abdominal hysterectomy (patient’s logical choice). She was in Dr Geetanjali’s office a few months later and while we were discussing fibroids remarked happily: “I had the mother of fibroids!”

18.11.15
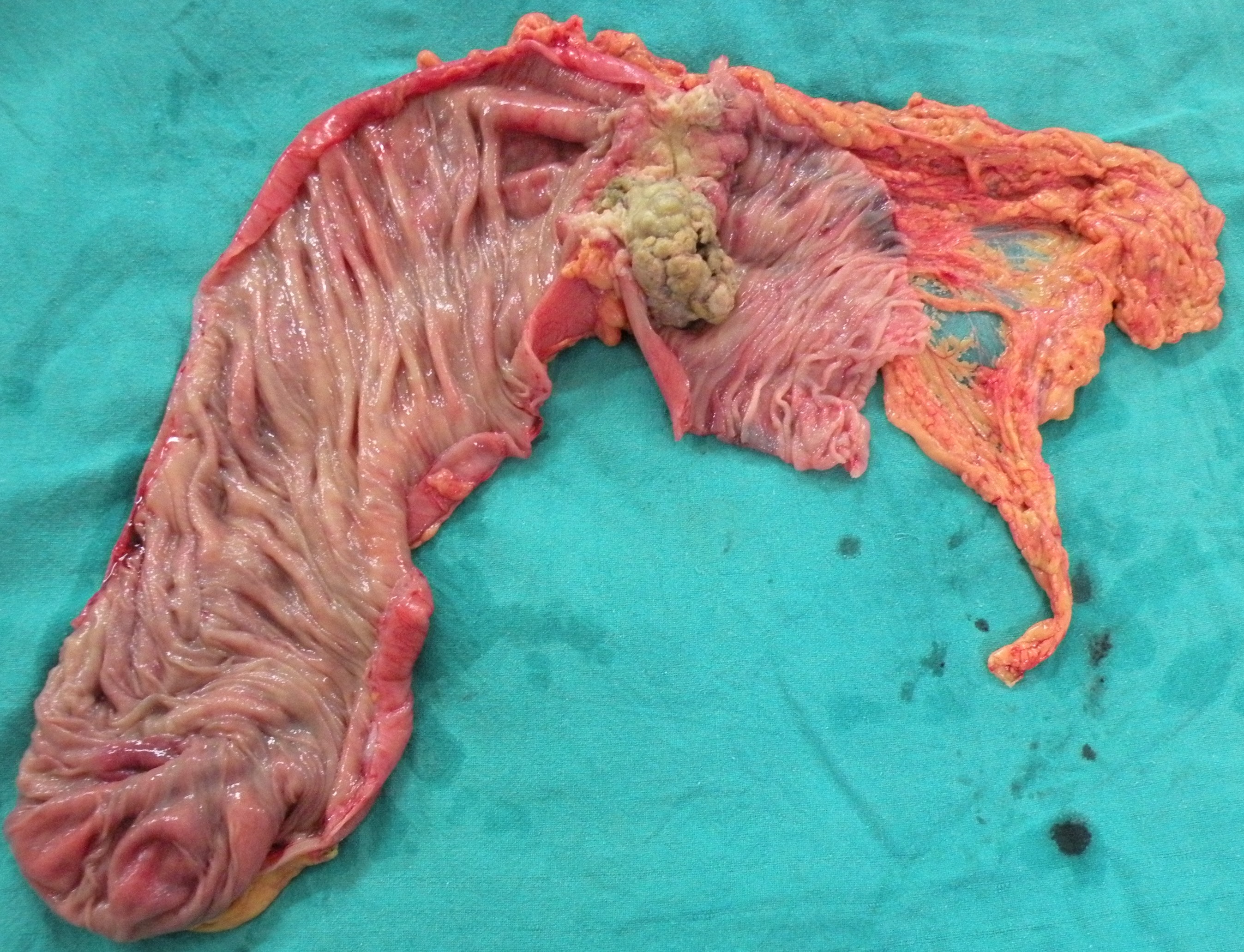
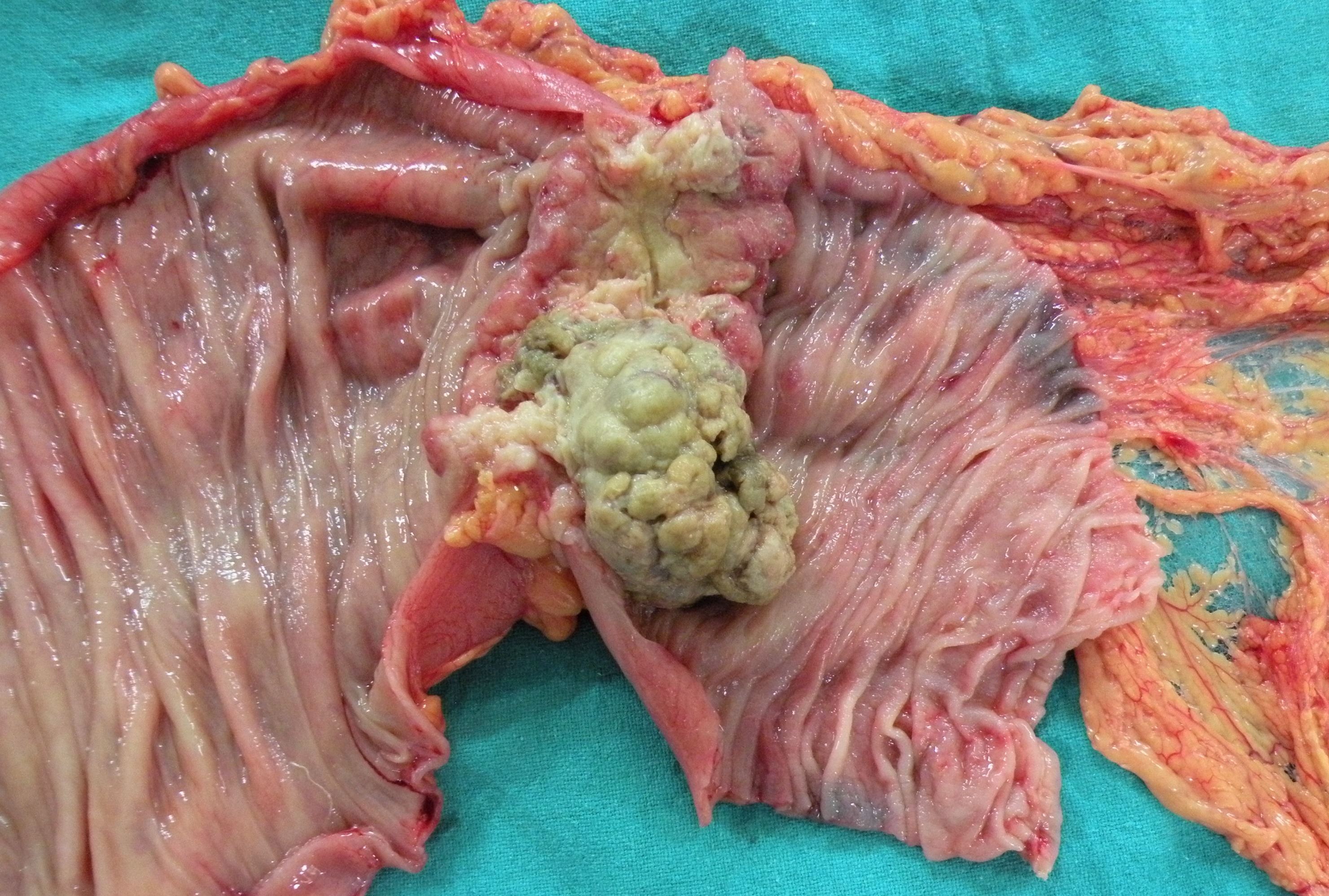
A distal radical gastrectomy in a 60 years old man (chronic smoker for a long time) for distal cancer causing gastric outlet obstruction. The tumor turned out to be bigger than expected (CT had only reported wall thickening of 2 cm), breaking through serosa and involving multiple lymph nodes above and below the pylorus, besides adhesions posteriorly with the pancreas. 

26.9.15
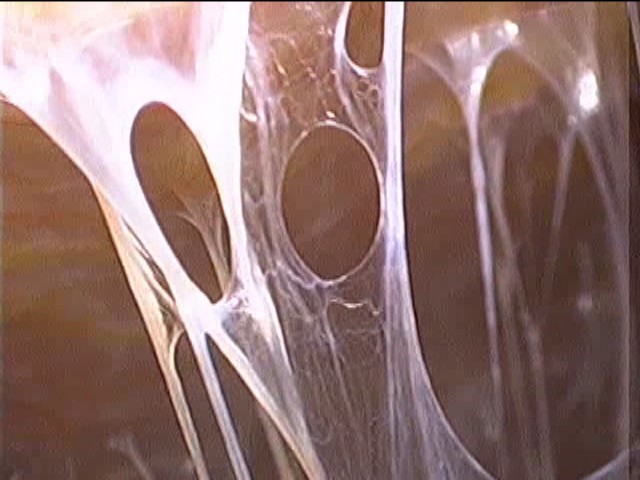
Dense adhesions around the liver and gall bladder, including violin-string type (Fitz-Hugh-Curtis), made lap chole difficult, but the procedure was eventually satisfactory.
Another lap chole (Angoori devi, c/o Kammo) was complicated by falling oxygen saturation levels near the end of the procedure. A C-arm image showed left pneumothorax, which necessitated a chest tube insertion and overnight stay in ICU for ventilation to expand the lung. The anesthetist’s explanation was the pneumothorax was due to diaphragmatic injury at surgery!
7.10.15
Visit to Chandigarh with dr Sushil Mittal for purchase of ETO sterilizers for operation theatres by the health systems corporation. Besides this purchase, another momentous decision was taken here. A suggestion given by dr Sushil Mittal was to stop using cars and instead use the bicycle for visits to the college and back. This proposal was immediately accepted and it was decided that both of us from now onwards will use bicycles rather than cars as far as possible.
18.10.15
Attended a CME on hepatobiliary and pancreatic surgery at Ludhiana (organised by dr Kuldeep Singh) along with dr Grover and Dr Jagga.
24.10.15
A laparotomy for abdominal pain and obstruction due to adhesions, following a traumatic bowel perforation which was treated in DMC with a resection-anastomosis and an ileostomy. This was followed by ileostomy closure, which was complicated by a fecal fistula, which had healed with conservative treatment. But the patient continued to experience pain and distension.
At exploration, extensive bowel adhesions had to be lysed, besides excising the ileo-cecal segment which was too densely adherent with an underlying thick-walled chronic abscess.

abscess cavity

ileum opened up with abscess cavity above
31.10.15
An intended Whipple resection for a cancer of the head of pancreas ended up in only a palliative biliary bypass procedure (cholecystojejunostomy). Once the pancreas was mobilized, the tumor in the head of pancreas was found to be densely adherent with the portal vein and also the gastroduodenal trunk (This was suggested by the CT scan, but still it was decided to go ahead with resection if possible).
4.11.15
An extended right hemicolectomy for a big palpable cancer in the transverse colon in a 60 years old female. The peglec bowel preparation by the residents had resulted in gross distension of all bowel proximal to the tumor, making surgery difficult and prolonged. However, the anastomosis with staples saved some time.
A forgotten ureteric stent develops a stone in the bladder, Anandpur sahib VVIP duty, a lap nephrectomy and an Ileal pouch anal anastomosis
Posted on: September 13, 2015
18.6.15
Attended the 350th year celebrations of founding of the city of Anandpur Sahib, as a member of the VVIP medical team. The PM was supposed to attend the same, but instead the home minister Rajnath Singh came.
24.6.15
Laparoscopic nephrectomy in a young (23 years old) female for non-functioning hydronephrotic kidney (congenital PUJ stenosis). The procedure was rather easy.
1.7.15
IPAA made in a young male, who had earlier (on 11.8.14) undergone subtotal colectomy for severe fulminant ulcerative colitis not responding to medical therapy. The completion proctectomy was difficult. The stapled ileal pouch anal anastomosis was not satisfactory, so a proximal ileostomy was added.
4.7.15
Completion thyroidectomy in a 35 years old female following a right thyroid lobectomy and the pathology reporting a papillary carcinoma. Surprisingly, the pathology report this time was not malignant.
8.7.15
A day of difficult cholecystectomies. The first was a young female with a thick-walled mucocele which had to removed piecemeal, after its cystic duct was ligated. The second and third were middle aged females with choledocholithiasis for which they had undergone ERCP, stone extraction and biliary stenting. The gallbladders too were thick-walled and the cystic ducts wide, needing ligation with no 1 vicryl suture.
Summer vacation from 9 July to 16 August
7.8.15
Court evidence at Dhuri through a warrant rather than a summon for expert evidence! 12.8.15
12.8.15
Attended the first meeting of the newly constituted Punjab chapter of ASI at Jalandhar.
22.8.15
Failed to create extraperitoneal space in an attempted TEP repair of inguinal hernia due to obesity and poor muscle relaxation. Converted to open procedure.
12.89.15
A stone grown on a forgotten DJ ureteric stent. The stent had been there for more than 10 years. Both the stent and stone were removed via a cystostomy.



Neurilemmoma of the thigh, disseminated intraperitoneal hydatids, gangrenous perforated gallbladder with bile peritonitis, and a rare conversion to open chole.
Posted on: June 21, 2015
16.5.15
An unexpected finding at an apparently routine lap chole. The gallbladder was found to be perforated and gangrenous with lot of bile in the peritoneal cavity. Postoperatively patient continued to have tachycardia and some fever for 2 days, then settled.
27.5.15
An attempted lap chole in a 45 years old lady failed due to dense adhesions from previously laparotomy (long midline incision going right up to xiphoid, done for liver laceration 2 years back). Even at open cholecystectomy, the procedure was difficult.
3.6.15
Disseminated intraperitoneal hydatid cysts in an 85 years old male presenting with abdominal masses and fever. The cysts had become infected and developed thick walls which were densely adherent all around. All cavities cleaned of pus, debris and grape-skin like small cysts, and drained with wide bore tubes on both sides. postoperatively, drained thick dark bile on second day, and continued to drain for many days.
10.6.15
Neurilemmoma of the thigh, recurred after excision twice. 50 years old female. The big tumor was excised along with sacrifice of the medial cutaneous nerve of the thigh from which it was arising, and along with some of the fascia lata with which it was adherent.