Hepaticojejunostomy for BDI, wrongly diagnosed cystic pancreatic tumor, twisted ovarian cyst, GB empeyma, TEP repair, ABSI conference and a free medical camp
Posted on: June 9, 2013
25.4.13
BDI (at lap chole 18.3.13) repaired by Roux-en-Y hepaticojejunostomy. High (type III) injury at hilum, both ducts (right and left hepatic) exposed at hilum, left duct exposed further by lowering the hilar plate and enlarging its lumen to avoid stricture later. Follow up so far satisfactory.
6.5.13
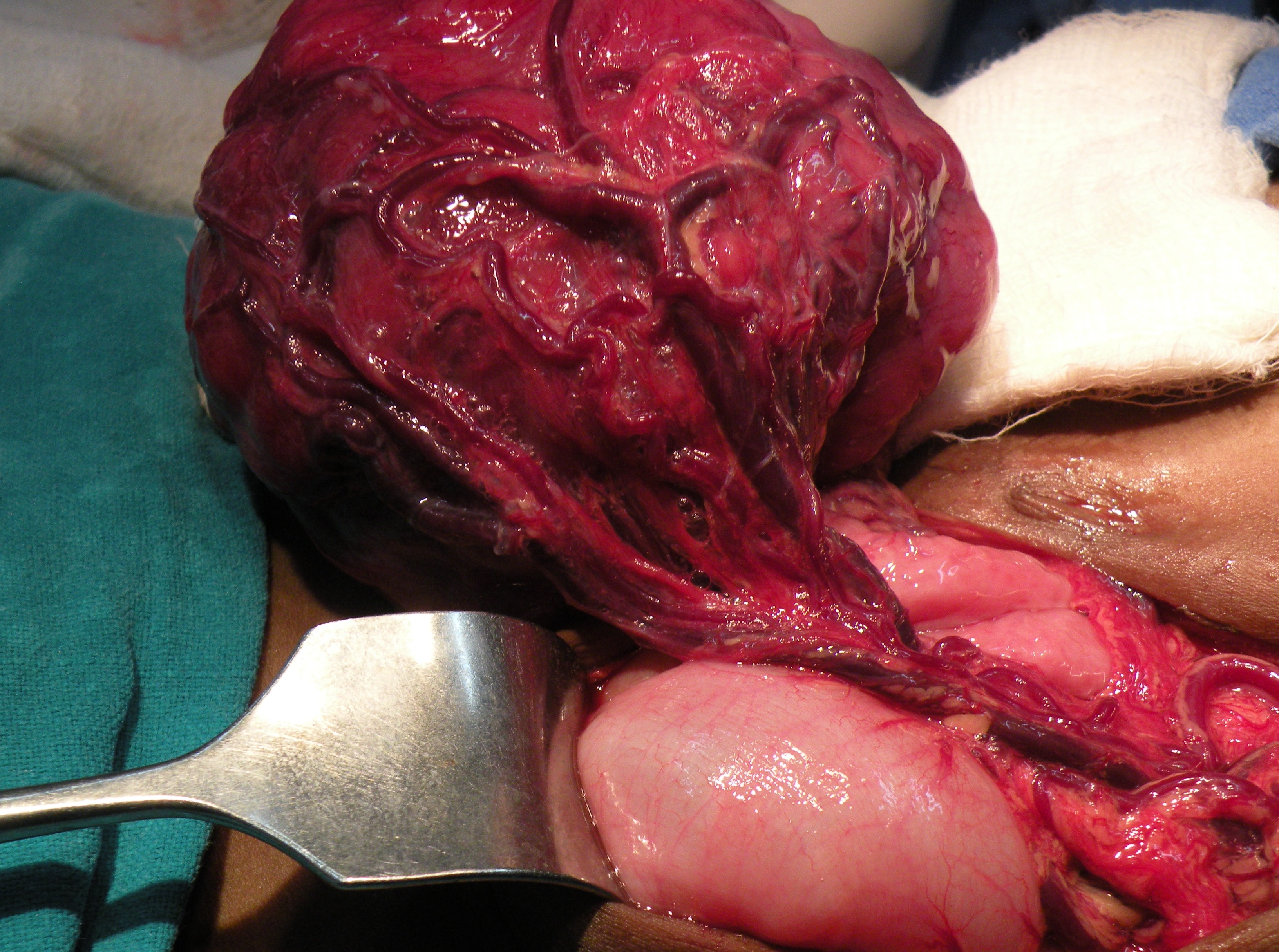
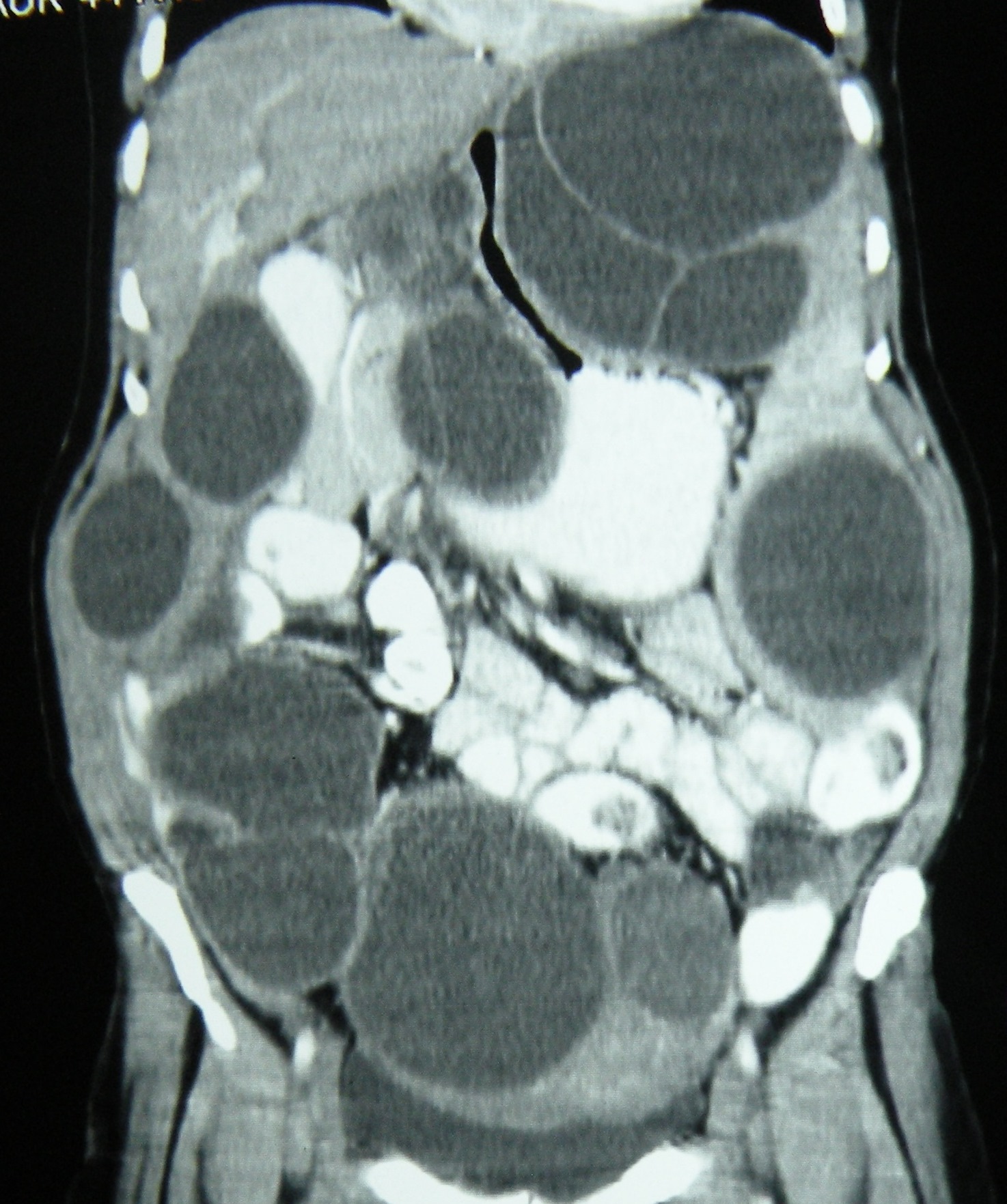
A 25 years old female, with a CT diagnosis of hepatic hydatid taken up for laparotomy. Turned out to have a retroperitoneal cyst on exploration, and on further dissection was found to be arising from the head of pancreas (?cystic neoplasm of pancreas). A large amount of haemorrhagic fluid aspirated and a lot of degenerated material evacuated from within the cavity, the walls of which were also excised. May need resection of pancreas later, depending on the biopsy report.
9.5.13
A difficult lap chole in a young Nigerian (undertrial here for drug trafficking) male, with a thick walled empyema, neck of gallbladder ligated, and the gallbladder removed piecemeal.
13.5.13
Lap chole in a young (20 y o) male with spherocytosis. Will have splenectomy later.
16.5.13
A young unmarried girl from gynae (dr khushpreet’s case) with bilateral ovarian cysts, for laparoscopic removal. Large left cyst had twisted, the thick walls removed piecemeal, the right one was a small paratubal cyst, removed intact.
17.3.13
Attended the annual ABSI conference at PGI Chandigarh. Lectures mainly on breast reconstruction.
30.5.13
TEP repair of right inguinal hernia in a tall young (25) rural man, addicted to bhukki and alcohol. Complete sac, transected and reduced.
2.6.13
A free medical camp organized by Akal academy, held at Cheema sahib in Mansa district. Examined more than 50 patients with surgical problems. Will be taken up for free surgery.
6.6.13
Displaced Cu-T found, at laparotomy, to lie embedded in the omentum part of which was excised. An earlier attempt to find the Cu-T at laparoscopy had failed on 22.2.13.
Lap chole 45 F, easy. Small Rouviere’s sulcus.
Appendix stumpitis, branchial cyst, mesenteric fibromatosis, and a femoral hernia
Posted on: April 22, 2013
5.4.13
30 years old female, thought to have pain right lower abdomen because of a TO mass (on US), turned out to have no such mass, but a stump of appendix (left after previous open surgery) – removed laparoscopically.
11.4.13
A large branchial cyst in a 15 years old girl, excised. Contents purulent, hence the pain and sudden enlargement recently.
 <
<
 </a
</aLaparotomy for a solid mass in 12 years old boy – turned out to have a solid big mass from mesentery, attached to ileum, which had to be resected along with the mass. The biopsy report was mesenteric fibromatosis.
 >
>
Case Reports in Surgery
Volume 2013 (2013), Article ID 569578, 3 pages
http://dx.doi.org/10.1155/2013/569578
Mesenteric Fibromatosis Presenting as a Diagnostic Dilemma: A Rare Differential Diagnosis of Right Iliac Fossa Mass in an Eleven Year Old—A Rare Case Report
Abhinav Mahajan, Mohinder Singh, Anoop Varma, Gunjeet Singh Sandhu, Malwinder Singh, and Rupesh Nagori
22.4.13
Femoral hernia, strangulated, in a 70 years old female. Could not be reduced through lower incision. A lower midline laparotomy added, loop of strangulated terminal ileum released, and an end to end anastomosis made after resection. Hernia repaired from below with ethilon 1-0 interruptted sutures.
Failed attempt to find displaced copper-T, lap excision of renal cyst, a Dutch lady’s lap chole, appendix abscess in a 60 years old woman,a partial bile duct injury and intraperitoneal hydatids.
Posted on: April 4, 2013
- In: operations
- 1 Comment
22.2.13
A laparoscopic attempt to find a displaced copper-T failed. Later found at open surgery to be concealed in the omentum, which had completely wrapped itself around the copper-T.
4.3.13
A wrongly diagnosed ovarian cyst (young unmarried woman 22 years old) went for a laparoscopic removal, but at operation, it was found to be too big and more solid than cystic, so converted to open removal. Path report – Leydig Sertoli tumour.
7.3.13
Bilateral TEP repair of inguinal hernia in 45 years old man, smooth and simple.
Laparoscopic excision of symtomatic renal cyst in a 62 years old man was easy.
Lap chole in a 50 years old Ducth lady was difficult. The gallbladder was packed with big stones, all had to be removed first, then chole was easy.
14.3.13
Laparotomy in 60 years old woman with appendix abscess and an autoamputated appendix. Pus drained, and appendix removed.
18.3.13
Most difficult lap chole. 50 years old female, dense omental adhesions took more than half an hour, dense adhesions with duodenum took more than one hour, then a big stone in neck had to be removed to gain access to calots triangle, stones removed but cystic duct was misidentified for dense adhesions in middle of gallbladder fossa and cauterised to leave a hole in it, which drained bile postoperatively for a long time. ERCP failed to identify CBD and stent it. The bile duct injury was repaired by Roux-en-Y hepaticojejunostomy (left duct approach) on 25.4.13. The upper CBD had disappeared (cautery damage?), leaving the two hepatic ducts open at the hilum. Postoperative recovery was entirely satisfactory, so was the follow-up.
4.4.13
Intraperitoneal and retroperitoneal hydatids in a 55 years old woman, all excised over a period of more than 2 and 1/2 hours.

GB agenesis, vasovasostomy etc
Posted on: February 18, 2013
15.1.13
A lap chole in a 60 years old man with empyema tested skills. GB cut open and removed in pieces after removing the stones. The gallbladder ligated at its neck without identifying the cystic duct which could not be identified. The neck ligated again with preformed catgut loop (ethicon), but leaked bile for some days through the drain, eventually drying up.
28.1.13
MRM of mother-in-law’s cancer (medullary) of breast. L nodes reported negative.
4.2.13
Abdominoperineal resection for an anal canal cancer which did not respond to Nigro’s chemoradiation therapy. 60 years old man. The perineal wound had apparently healed nicely when he was discharged after 25 days. However, a week later, the perineal wound gaped (previous radiotheray, delayed healing?), and was resutured.
5.2.13
GB agenesis in a 25 years old male (bhukki addict) presenting with pain upper abdomen and US reporting gallbladder stones. No gallbladder could be found, after removing adhesions of omentum and colon mesentery in the gallbladder fossa.
11.2.13
Vasovasostomy in a 50 y o man who wanted to have children again.
18.2.13
Open CBD exploration in a 50 y o female (relative of dr Rama, my classfellow) for a big calculus (primary) in the CBD .Had an earlier endoscopic papillotomy but the stone could not be removed, and a stent had been placec. Today, a single big stone removed from CBD. No stone was found in the gallbladder removed.

13.12.12
TEP repair of inguinal hernia on a 60 years old man, the inferior epigastric pedicle got detached but no further problems with dissection.
18.12.12
Held a clinical meeting in ME cell of the college, wherein two rare presentations of tuberculosis of the vertebral spine were discussed. The cases were presented by Dr BL Bhardwaj, professor of medicine.
15.1.13
A very difficult empyema of gallbladder in a 60 years old man. Lap chole by opening the gallbladder first, emptying it of stones, and then fundus first dissection, and then ligating at the neck.
19.1.13
Herniotomy in a one year old female child with right inguinal hernia. The contents were the ovary and fallopian tube, saw this for the first time.
21.1.13
Trichobezoar removed from the stomach of a 5 years old female child.


Plexiform neurofibromatosis
Posted on: November 5, 2012
A huge neurofibroma, a part of von Recklinghausen’s NF, excised from the back of a 25 years old lady.

25.10.12
Re-exploration laparotomy for an obstructed gastric outlet, after laparotomy 3 weeks earlier by residents, in a young (20) male, with transection of duodenojejunal junction following trauma in a RTA. After the duodenal continuity was restored with a sutured anastomosis, a GJ had been added!. The patient continued to have more than 500 ml of bilious NG aspirate, and on removing the tube once, had some bilious leak from the abdominal wound, suggesting anastomotic leak, so the tube was put back in. At operation, the the DJ anastomosis was found to be strictured, and was dilated through an enterotomy with foley balloon and metal dilators, and the GJ was converted to RYGJ.
1.11.12
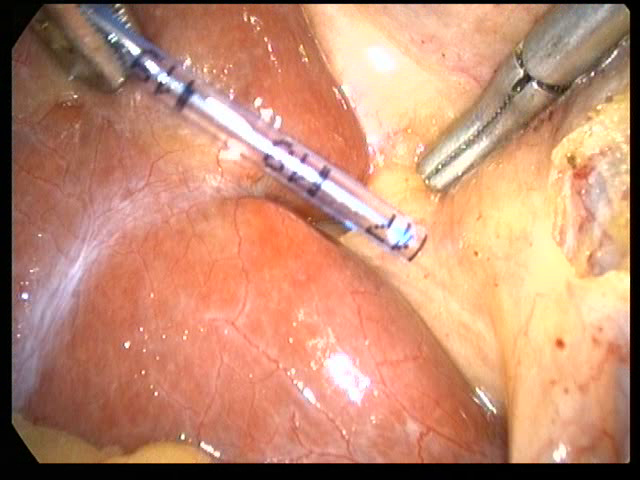
At lap chole, measured the dimensions of a Rouviere’s sulcus with the help of a feeding tube marked in centimeters, as a part of studying the anatomy of Rouviere’s sulcus as seen during laparoscopic cholecystectomy.

NCASICON at jalandhar – attended for two days : 8 and 9 september. Saw dr Chanjiv and others there.
13.9.12
Open prostatectomy for a huge (150 g) prostate who presented with hematuria. Postoperatively, developed clot retention, and had to be reopened.
Undescended testis in a 2 years old child- no testis found – anorchia.
20.9.12
Closure of ileostomy for a patient of Crohn’s disease who had presented with obstruction and residents excised a segment of ileum and had done an ileostomy. Patient on azathioprine by GE.
Revision of GJ into Roux loope GJ. An older patient who had presented in 2006 with GOO and had TVGJ performed. Now continued to have pain and vomiting intermittently. At operation, had stenosis of both limbs of GJ, which was revised into Roux-en-Y GJ. Did well thereafter.
21, 22 sept
attended SELSI hernia conference at Gwalior along with Dr Sushil Mittal and his team.
28.9.12
Abdominoplasty (assisted dr GP singh) for huge abdominal apron hanging down in a 45 years old female. Persisted with seromas for a long time.
3.10.12
dr Khushpreet’s case – laparoscopic excision of right ovarian cystic mass and left hydrosalpinx.
4.10.12
TEP repair of LIH in a 30 years old male.
11.10.12
TEP repair bilateral hernias 70 years old male. Had seromas both sides postop.
15.10.12
Mahesh Kumar, obese 50 male, admitted with severe pain in OPD. Very difficult lap chole due to obesity, gangrene of fundus of gallbladder, and thick walls making grasping impossible. Calots anatomy not clear. Ligated at lower part of gallbladder and then the suture used to retract the gallbladder further, then Calots defined. Took 4 hours.
22.10.12
Parotidectomy superficial for parotid duct stone and chronic sialadenitis, and stone not palpable intraorally.


9.8.12
Two clipless lap choles – the cystic duct and artery sealed with harmonic scalpel.
20.8.12
An abdominoplasty – assisted Dr GP Singh, the plastic surgeon. Dr Jagga’s patient – a young (25) female, who got a huge divarication of recti after delivery of her baby. The recti were plicated with 3 layers of vicryl.
30.8.12
Two TEP repairs for RIH – both easy and enjoyable.
3.9.12
Thyroid lobectomy (right) for a deep seated nodule of right lobe. 55 years old female (c/o dr BL Bhardwaj). Hoarseness of voice persisted.
Prostatectomy (freyer) for a 120 grams huge prostate – easily shelled out – in a 60 years old. Haemostasis secured with sutures.
Billroth II, diagnostic laparoscopy, and a series of difficult empyemas of gallbladder with fundus first dissection
Posted on: August 8, 2012
26.7.12 A huge duodenal perforation, closed by residents on 20.7.12, releaking. Young male (20 yrs old poor bhaiya). Explored to find a large perforation and posterior wall of duodenum stuck to pancreas. Mobilised with difficulty and duodenal stump closed. Billroth II type resection and GJ done. Duodenal stump blow out on 5th PO day.
2.8.12 diagnostic laparoscopy in a young (25 yrs old) male from Patran with chronic abdominal pain. Patient of dr Parmod Mittal. Endoscopy in 2011 showed some ulcerations in terminal ileum and ileocecal area – so took ATT for a year or so, but abdominal pain still persisting. At laparoscopy, had adhesions from previous open appy in RIF- these were divided. Running of all small bowel showed no stricture. In the left flank, was an omental band, adherent down in the pelvis; this was released.
5.8.12 four lap choles, 3 of which turned out be very difficult. The first one, an old blind lady (60 yrs old)- While dissecting with hook posteriorly, some bile leak was observed; changed gears to do the fundus first chole and the gallbladder ligated at its neck by no 1 vicryl loop. Drained bile tru the drain. ERCP next day revealed leak from CBD near CD-CBD junction. Stented – the drain dried up in 2 days. The second turned out to be an empyema unexpectedly. Was a younger patient (40 years female) and there was no sign of difficulty preoperatively. But it was a thickwalled empyema. Cut open to remove pus and stones. Ligated at neck. Third one was easy. The fourth againd turned out to be empyema. and same process was repeated.
