6.3.14
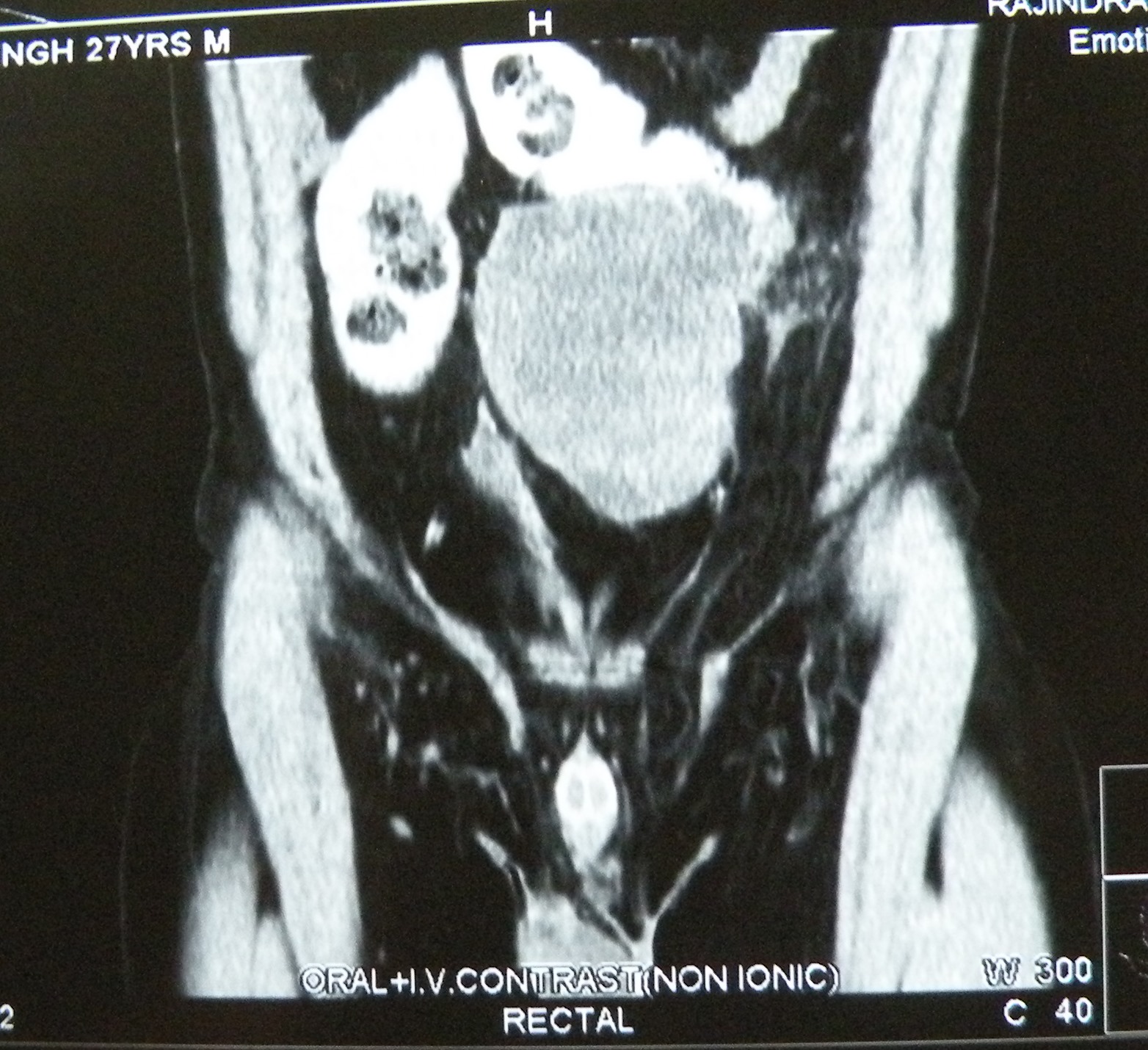
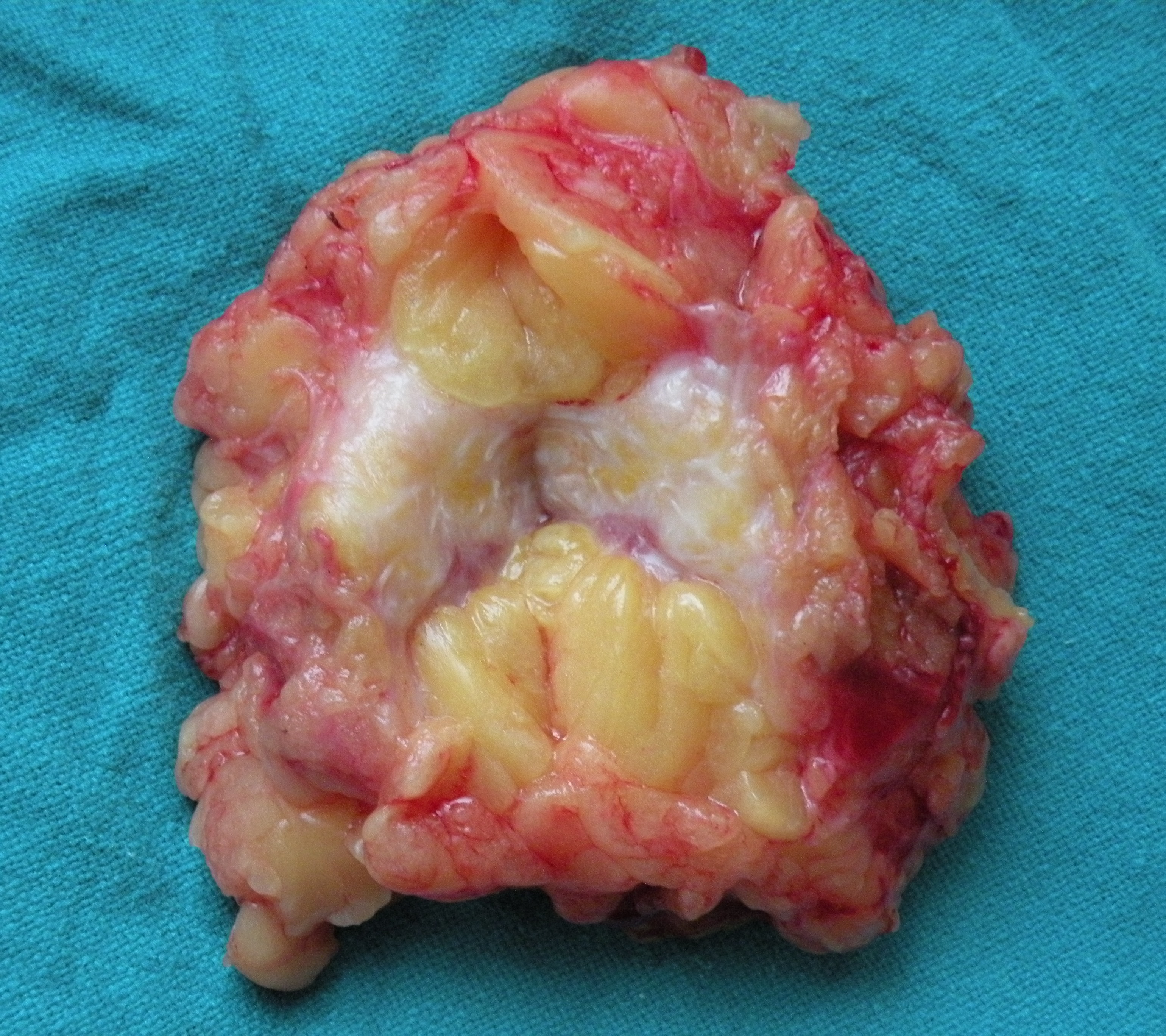
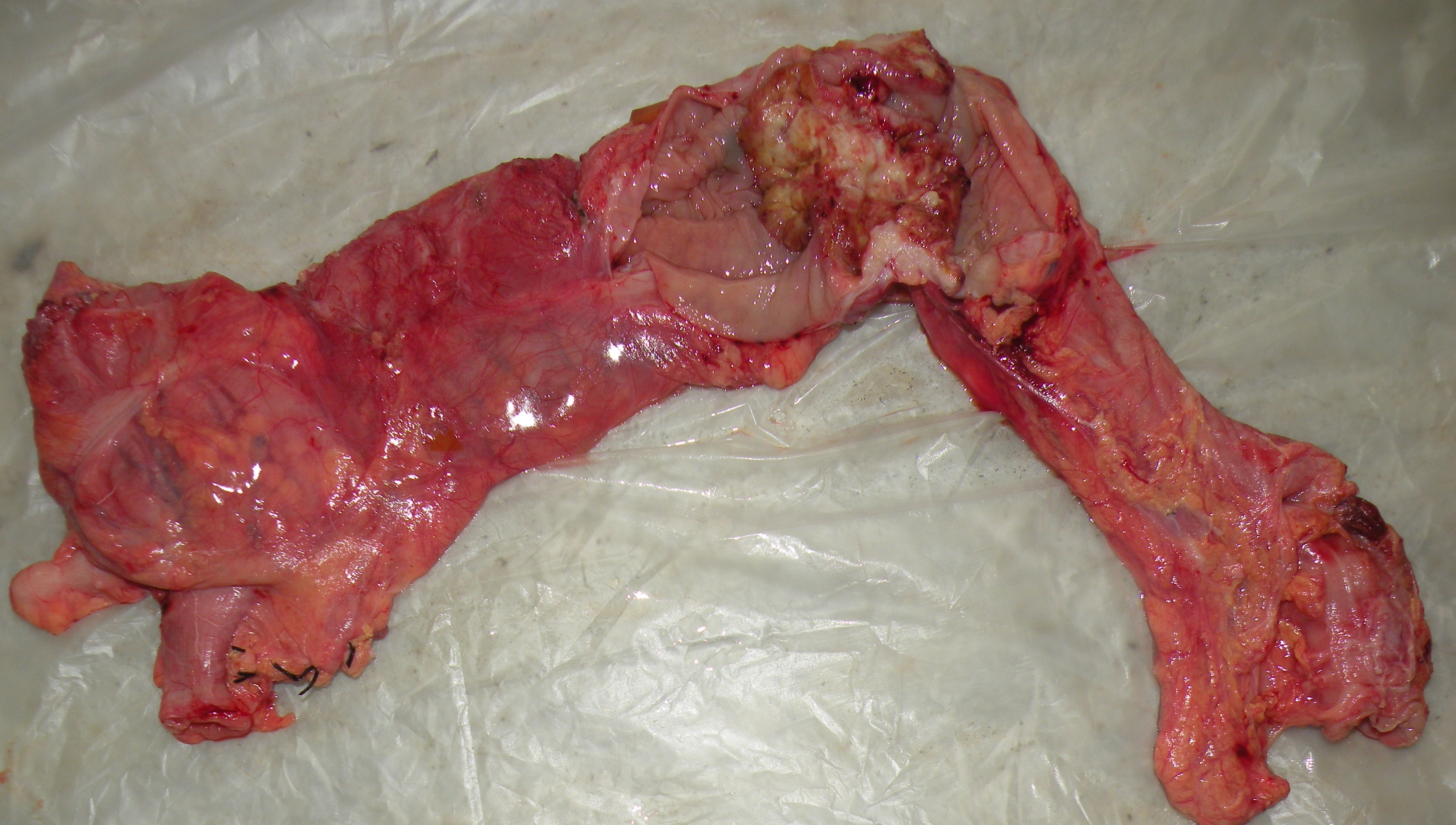
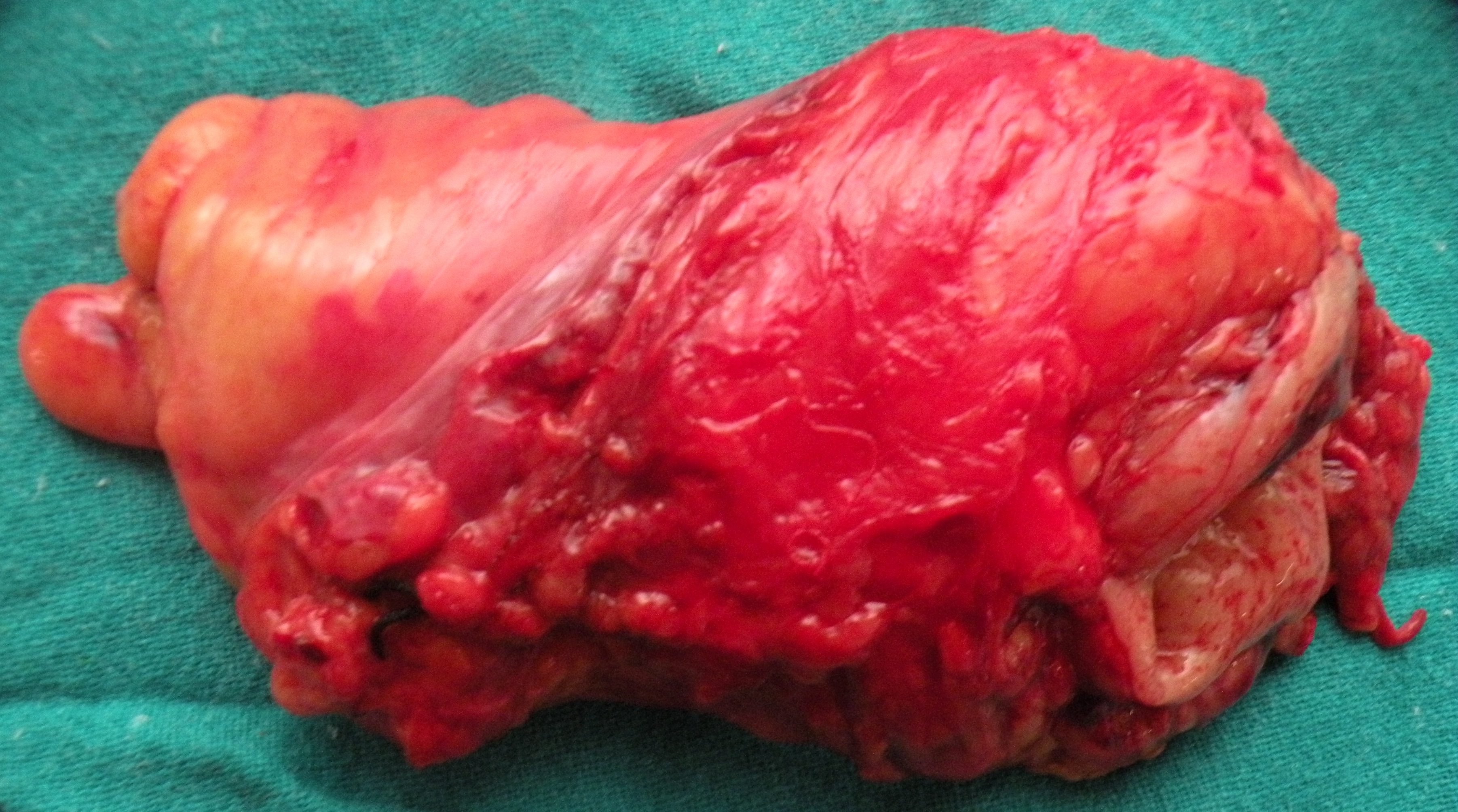
A 27 yeas old male, HCV positive, presented with a mass (15 cm across) in the left lower abdomen, and found to have an undescended testis on examination. AFP and HCG grossly elevated. At exploration, the big tumour was found to be adherent to the sigmoid colon, which had to be resected along with the tumour.

An arteriovenous malformation on the forehead in a 22 years old man, previously incompletely excised in Haryana, excised again after ligating the feeding superficial temporal and other small vessels.


A breast lump in a 60 years old female, negative on FNAC and Core needle biopsy, excised widely. Cut section typically scirrhous.
Jejunal duplication and stricture, a pyelolithotomy, and a parotidectomy
Posted on: February 17, 2014
An unusual presentation for a small tubular duplication and stricture of jejunum causing obstruction in a 60 years old lady. The jejunal segment was excised and an EEA performed.
23.1.14
A difficult lap chole in 50 years old male (Bhupinder singh from kheri) with a thick-walled mucocele, removed piecemeal.
3.2.14
A pilonidal sinus (recurred after 7 years), in a 25 years old male (s/o Dr Avinash Gupta ortho), excised and sutured. close
5.2.14
Pyelolithotomy for a big staghorn stone left kidney, and a small impacted stone in lower calyx, removed through nephrolithotomy. 40 years old male with the other kidney nonfunctioning due to ureteric stone, drained through a nephrostomy tube, for later possible nephrectomy.
6.2.14
laparoscopic repair of a portsite hernia (through the umbilical port of lap chole 3 years back), repaired with proceed mesh.
11.2.14
MCI inspection in the college. The hospital turned 60 years old, the staff celebrated by cutting a birth day cake and having photos with the medical superintendent dr Sharda.
17.2.14
Superficial parotidectomy for a 4 cm mixed parotid tumour in a 30 years old female, investigated in PGI.
 13.1.14
13.1.14
Transverse colon cancer, an ectopic pregnancy and a strange looking Rouviere sulcus
Posted on: January 4, 2014
19.12.13
MRM for an a breast cancer with open excision biopsy done at Rajpura civil hospital, no record available.
An extended right hemicolectomy for a transverse colon cancer in a 55 years old male. The patient had an interesting history of left colectomy with ileostomy (closed later) in Columbia Asia hospital about 3 months back, and now reporting with features of colonic obstruction and endoscopically diagnosed colon cancer again, this time in the right colon. An extended right colectomy was carried out; however, the whole left colon seemed to be intact and there was no sign of left colonic resection.

20.12.13
A right tubal ectopic pregnancy had ruptured through leaving a small hole in the tube. The hole was loosely closed with 4-0 vicryl.
26.12.13
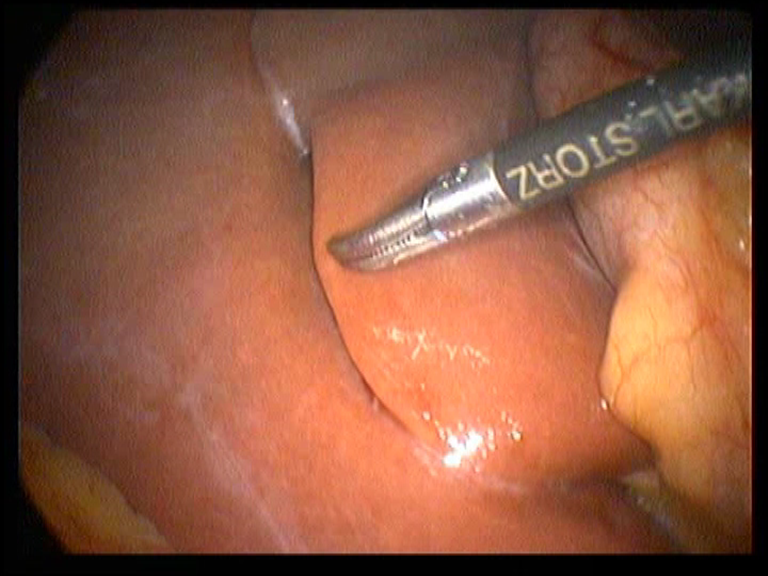
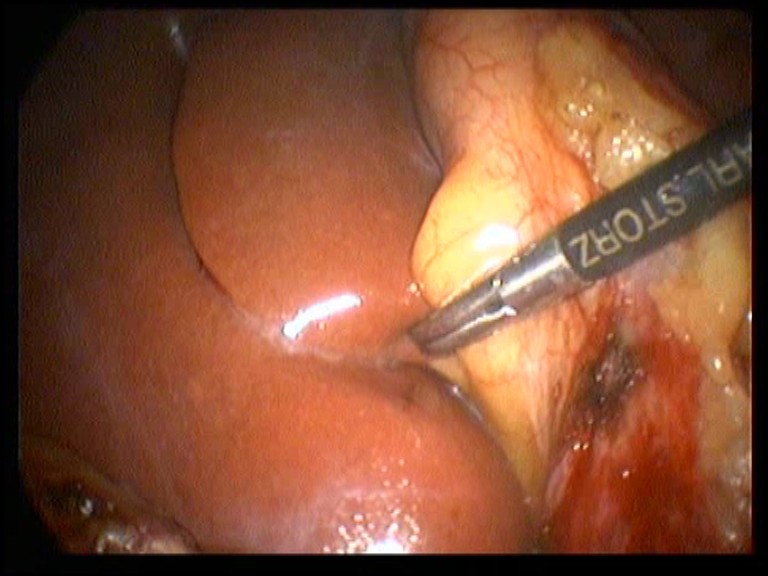
A strange looking Rouviere’s sulcus seen at lap chole.
A low rectal cancer resection, an ovarian cyst wrongly diagnosed, a stone impacted in a ureterocele, some difficutl lap choles and an open cholecystectomy
Posted on: December 16, 2013
28.11.13
a A mesenteric cyst (diagnosed clinically and on CT) turned out to be big ovarian cyst. easily removed at laparotomy.
An impacted stone in a ureterocele, removed through open cystostomy and meatotomy.
30.11.13
A difficult lap chole, thick-walled gallbladder adherent to live bed which bled furiously, controlled with packing.
16.12.13
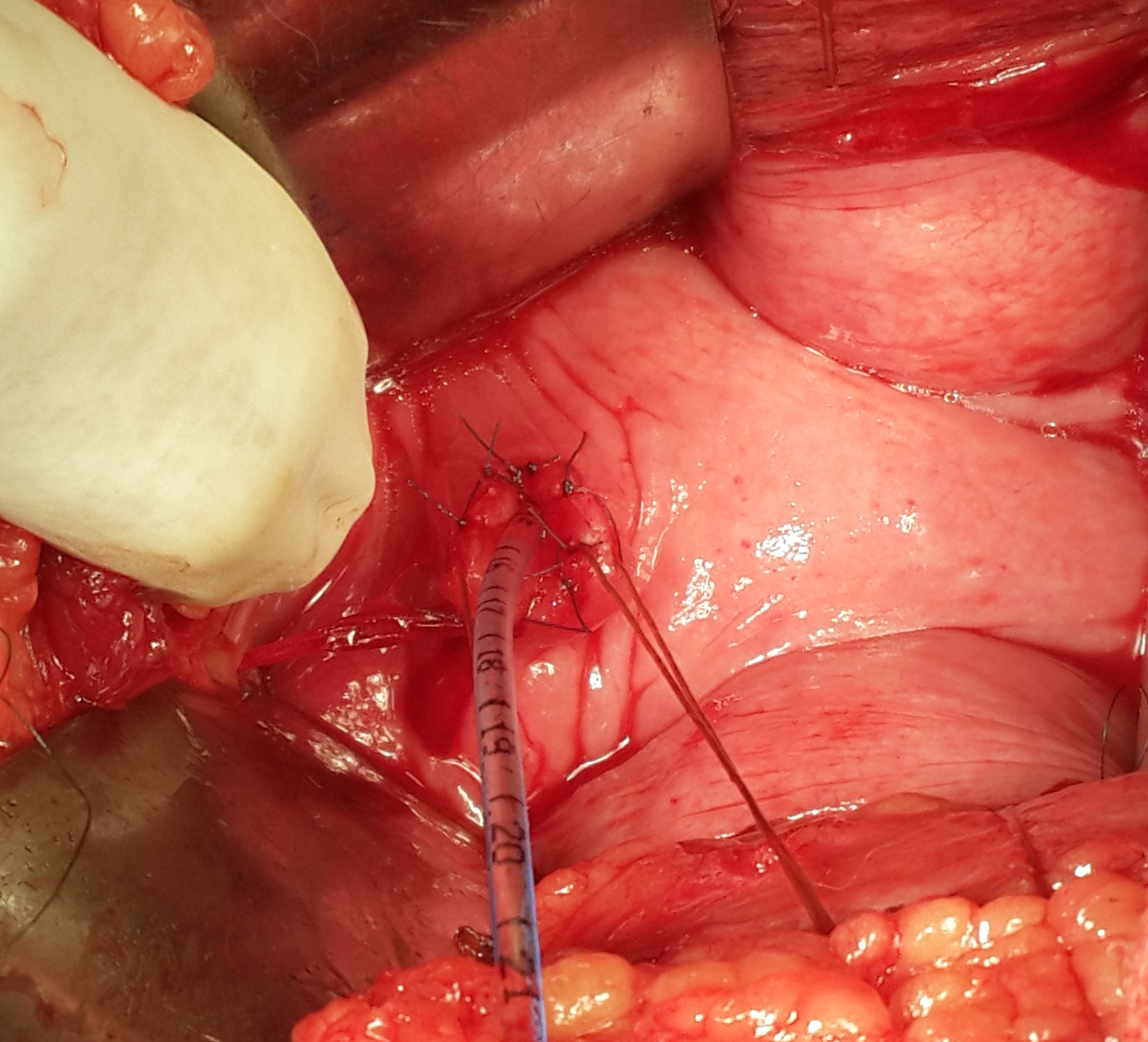
A rectal cancer (low) resected and a stapled anastomosis low in the rectum performed.

Posted on: November 19, 2013
18.11.13
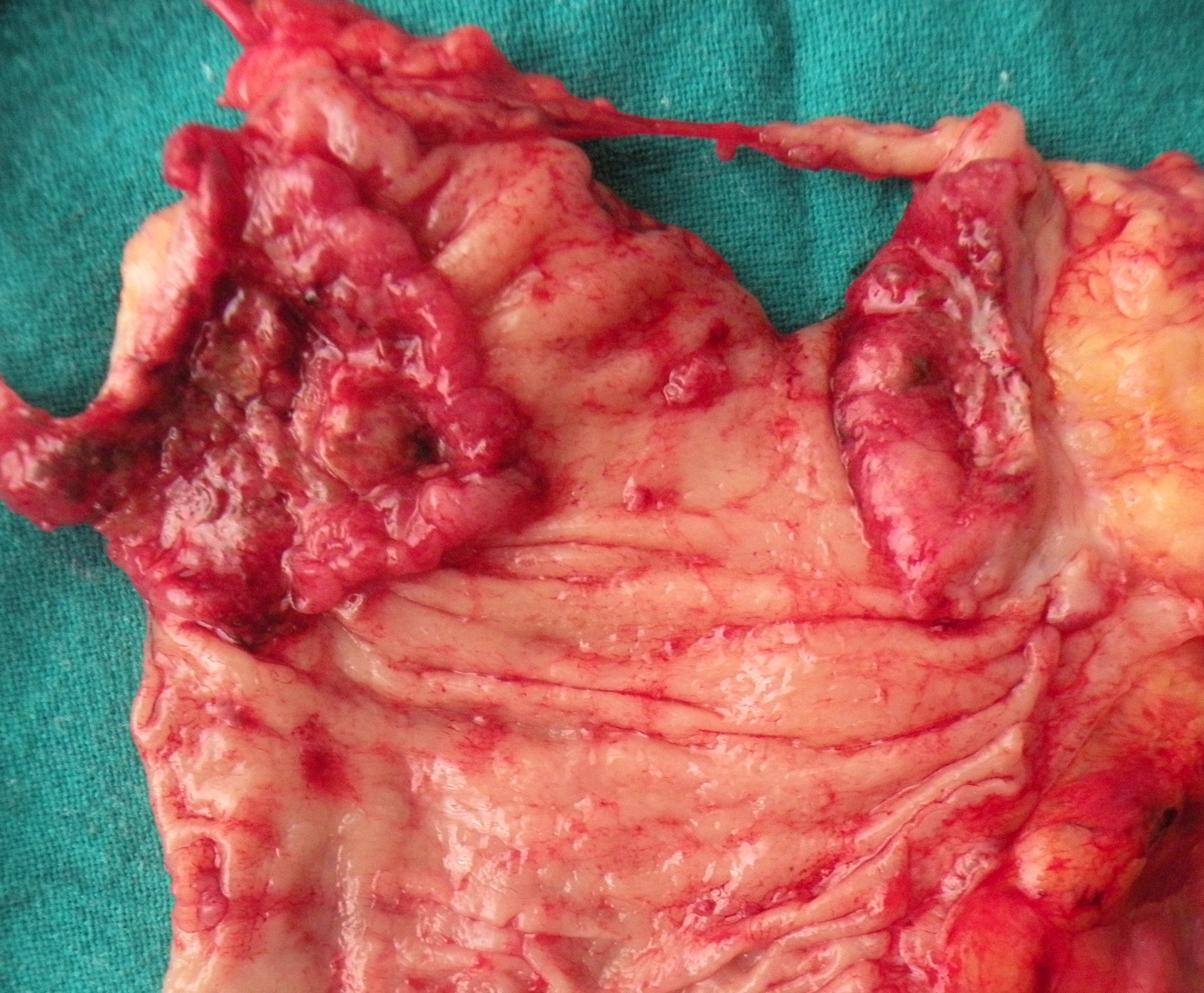
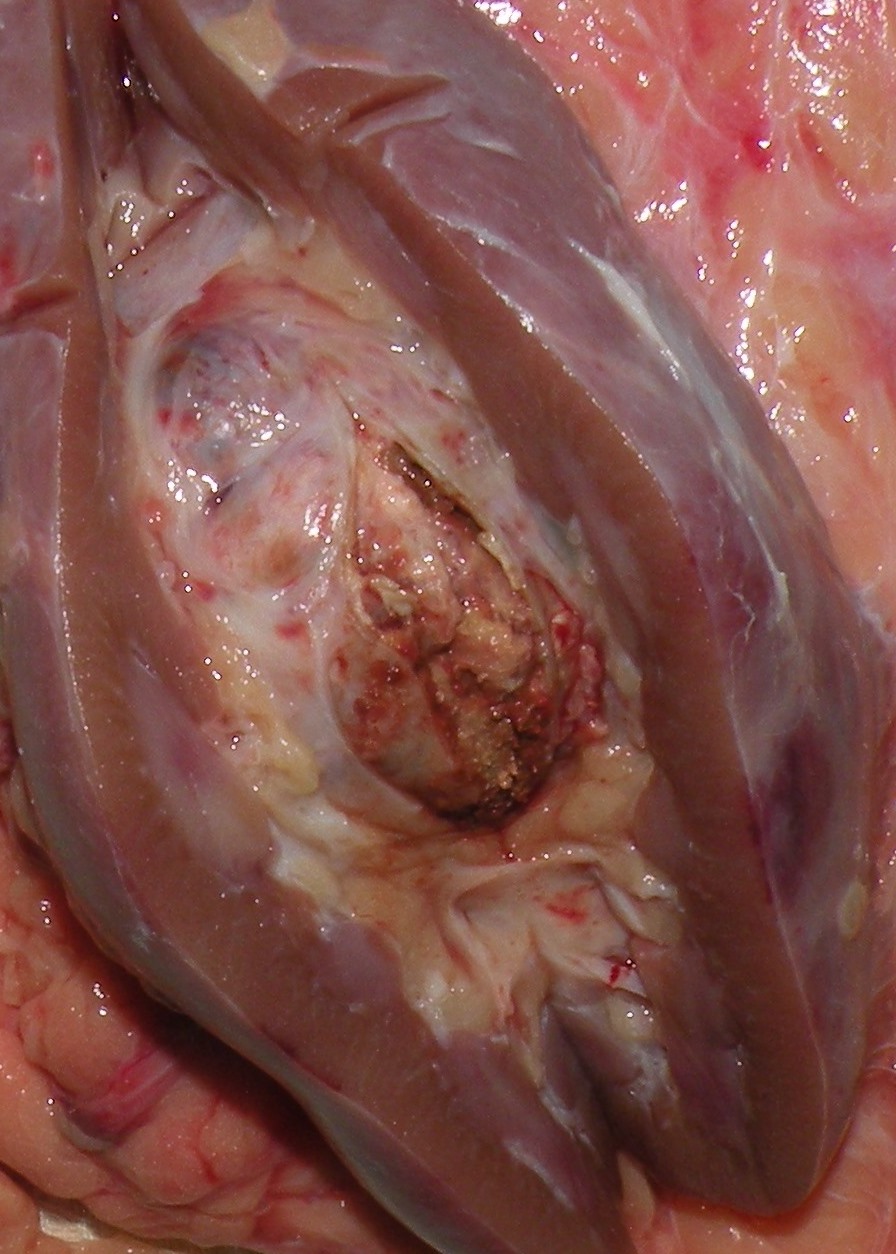
Anal cancer – Abdominoperineal resection in a young (30 years old) male patient for anal cancer, previously treated by chemoradiation. Specimen on cut section showed only a tight stricture like a dense scar, hardly admitting an artery forceps.

28.10.13
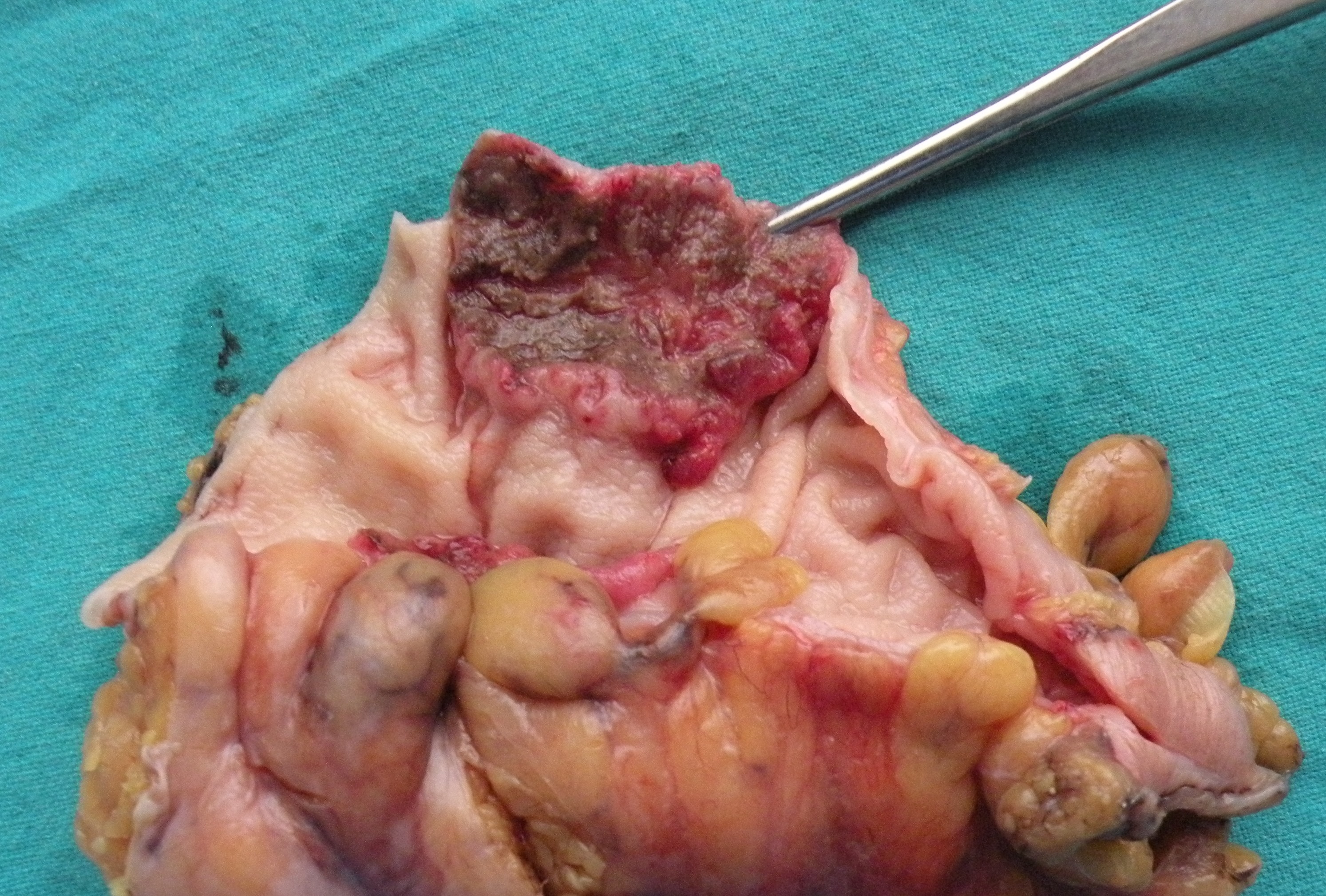
Laparotomy for intestinal obstruction due to strictures diagnosed on laparoscopy on 24.10.13. Resection of about 2 feet of midileum bearing the strictures, followed by EEA performed.
31.10.13
SILS (single incision lap surgery) performed for the first time appendicectomy in a young female. Difficult due to parallel instruments.
7.11.13 to 11.11.13
Attended a conference (ICS-IS) at Lucknow along with drs jagbir and sukhpreet.
19.11.13 A total laparoscopic hysterectomy using Harmonic and en-Seal (Dr Mohi’s case) performed in gynaecology department.
Anal cancer resected after chemoradiation, and a laparotomy for ileal strictures
40 years old male, poor emaciated addict (bhukki) with repeated attacks of subacute intestinal obstruction. At laparoscopy, some adhesions in right iliac fossa, but the real cause of SAIO was multiple strictures in the small bowel about 50 cm proximal to the ileocaecal junction. Some fluid in the pelvis, was sampled for lab studies, especially for tuberculosis.


24.10.13
Radical nephrectomy for RCC
Posted on: October 21, 2013
21.10.13
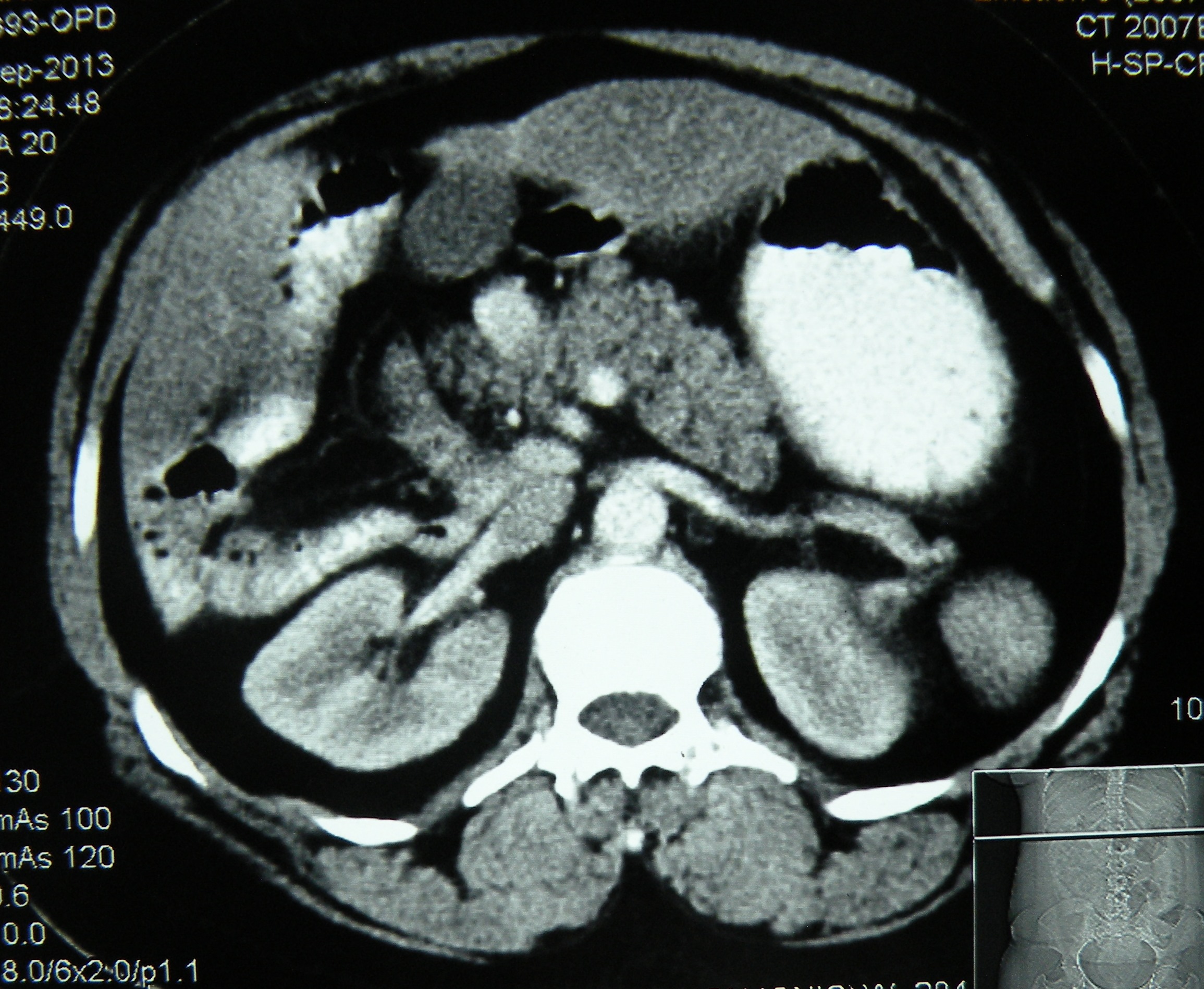
Radical left nephrectomy for RCC in the middle pole of left kidney. Patient a 45 years old man (c/o worker at dr Sachdeva clinic). Had one episode of haematuria and CT showed the tumour. Anterior approach, removed with perinephric fat intact. No lymph nodes palpable.

Situs ambiguous(heterotaxia) with gall stones, an ileal carcinoid? and bad encounters with chronic liver disease
Posted on: October 11, 2013
9.9.2013
A lap chole converted due to impossible access (previous laparotomies for ileal perforation peritonitis, then closure of ileostomy + dense perihepatic adhesions).
18-20 September, 2013
Attended a SELSI conference at Srinagar. Good workshop showing hernias, lap ureterolithotomy, lap pyeloplasty, lap nephrectomy, lap CBD exploration.
23.9.13
Laparotomy for long-standing history of intermittent colicky abdominal pain in a 40 years old male. diagnosed presumptively with tuberculosis of intestines, and treated with ATT without relief. A recent CT showed 2 ileal strictures. At laparotomy, the segment of mid-ileum bearing the 2 strictures was excised and EEA done. Biopsy surprise was carcinoid.
26.9.13
Encounter with CLD 1 – A very difficult lap chole ended up in conversion. CLD with previously low PTI and previously postponed several times. Presently all LFTs and PTI reported to be normal. A very thick-walled and adherent gallbladder dissection resulted in duodenal tear and prolonged oozing from liver bed. After conversion to open, bleeding controlled with pressure and suture of liver bed, and the duodenal tear repaired. But the patient ended up in ICU due to incomplete recovery from anaesthesia, and there, her LFTs deteriorated and she died on 5th postop day.
7.10.10
Encounter with CLD 2 – A 50 years old female admitted with acute cholecystitis, now settled. Previously known history of portal hypertension and bleeding varices controlled with sclerotherapy for last 2 years. LFTs in normal range now – Childs grade A. So taken up for lap chole and burnt fingers again. Big vessels all around the gallbladder and in Calots triangle. Opened up for bleeding in Calots area, not controlled by pressure laparoscopically. At open operation too, the bleeding from liver bed severe, suturing of liver bed led to further bleeding, compounded by a retractor injury to the liver bed. 2 abdominal packs and pressure controlled the bleeding, and patient closed with packs in place. The packs were removed 5 days later when the patient stabilized, but the packs were found to be getting infected, thought the bleeding had stopped. The patient continued to drain through the abdominal drain for many more days.
10.10.13
An interesting case of situs ambiguous (heterotaxic syndrome) presented with history of failed open attempt at civil hospital, Nabha to remove her gallbladder which could not be found by the surgeon. Imaging (US, CT, MRI) here showed a central liver, with gallbladder placed in the centre between the two lobes, polysplenia, truncated pancreas and dextrocardia. At surgery, the gall bladder was found just to the left of the falciform ligament. A difficult lap chole (due to dense adhesions with falciform ligament and omentum) was done, with the main operating port in the LUQ of the abdomen.

 published later in
published later in![]()
| CASE REPORT Year : 2014 | Volume : 4 | Issue : 3 | Page : 180–182 Laparoscopic cholecystectomy in situs ambiguous Anoop Varma1, Abhinav Mahajan1, Mohinder Singh1, Gunjeet S Sandhu1, Navkiran Kaur2, |
A rectal cancer anterior resection, a breast cancer extirpation, a couple of difficult lap choles converted, and a variety of ectopic tubal pregnancies
Posted on: September 2, 2013
28.7.13
Ruptured left tubal pregnancy, lap salpingectomy with bipolar forceps.
29.7.13 A similar tubal pregnancy, similarly dealt with.
3.8.13
Right tubal ectopic this time, looked like a solid tumour inside of which were the products – could this be the result of methotrexate treatment which had been given to the patient?
5.8.13
Difficult lap chole (Dr Mohi’s patient 50 F), converted to open due to a big impacted stone in the neck of gallbladder and the calot’s triangle frozen.
8.8.13
Another conversion of lap chole to open, this time a 50 years old male patient admitted with acute cholecystitis last week. At operation, a thick walled empyema and Calot’s triangle could not be dissected. Had a stormy postop period. First 4 days normal , but had pain and distension of abdomen on 5th PO day. ERCP showed CBD stones, which could not be removed (?impacted), and CBD was stented. Then had pneumonitis which gradually settled with antibiotics.
20.8.13
Massive gangrene small bowel. A poor gardener, 50 years old, was admitted with 7 days old history of intestinal obstruction, kept on conservative treatment at Rajan NH, was found, at laparotomy, to have distension and gangrene of nearly whole of the small bowel, excepting nearly 2 inches of proximal jejunum and 2 inches of terminal ileum, which were anastomosed after resection. Was referred to PGI for TPN and further care, then was lost to follow-up.
A chronic ectopic ruptured tubal pregnancy, forming a solid mass, removed piecemeal.
2.9.13
MRM for an advanced (skin fixity) cancer of left breast. Lymph nodes (not palpable clinically) were a fixed mass adherent with axillary vein.
Anterior resection for a rectal cancer middle rectum (60 M, dr Jagga’s case). Shocking start of the operation because of the nick (with cautery) to the left iliac artery while beginning the mobilization of the sigmoid! Closed with 4-0 prolene. Then smooth sailing. Total mesenteric excision and stapled anastomosis of the descending colon to lower rectum.
12.6.13
Thick-walled empyema of gallbladder, removed piecemeal.
19.6.13
Big perforation of duodenal ulcer in a 30 year old smoker. Could not be closed primarily, only plugged with omentum.
21 t0 24 june, 2013
Lots of operations performed in a free medical camp at Baru Sahib, Himachal Pardesh: 7 open cholecystectomies, 5 inguinal hernia repairs, 3 paraumbilical hernias, and 2 hydroceles.
11.7.13
Complications arising out of a difficult lap chole (c/o staff nurse, OT). Thick walled empyema and fibrosed Calot’s triangle, ligated at infundibulum. Removed piecemeal after more than 2 hours of effort. Had bleeding from omentum postop that had to be ligated at laparotomy.
17.7.13
Priapism of 4 days duration in a 70 year old man!. Partial detumescence achieved by aspiration of corpora cavernosa and by injection of saline norepinephrine solution.

18.7.13
An attempted TEP (60 years old man) failed because of intraperitoneal entry in the beginning itself, converted.
19.7.13
Court evidence at Pathankot, went via Jalandhar.
25.7.13
A tumour of undescended testis on the right side in a 23 years old man. Excised at laparotomy.
 <
<


