Author Archive
The cremasteric reflex
Posted on: May 10, 2015
The cremasteric reflex in the 7 years old boy with right-sided undescended testis was nicely captured in a short video clip by a final year medical student.
15.4.15 Right sided undescended testis, in a 7 years old boy, was found to be impalpable and not shown up on the ultrasound scan. However, on exploration by assistant professor (dr djs walia), was found in the inguinal canal and was fixed in the scrotum after mobilization.


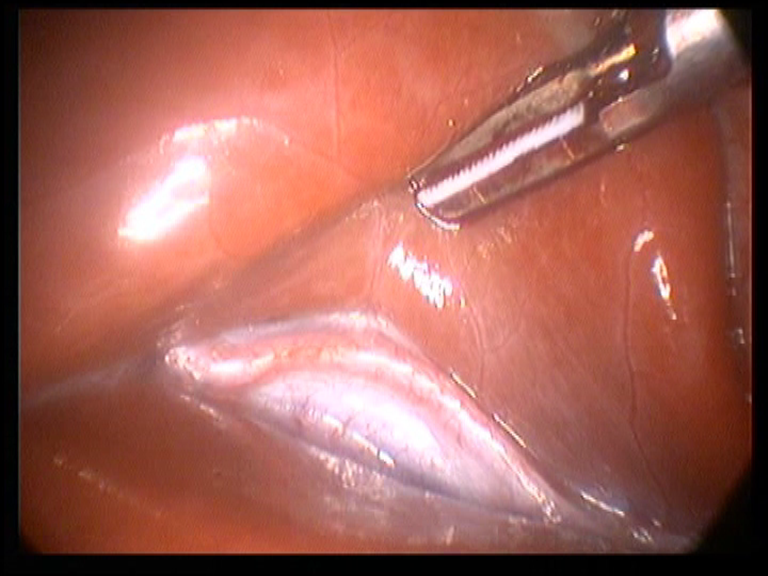
An 11 years old girl with torticollis – the tight band of the fibrosed sternocleidomastoid was released from its sternal and clavicular heads, and also from its mastoid attachment, using the harmonic scalpel.



A failed lap appy, a testicular tumor, an omental band causing intestinal obstruction and a lip swelling
Posted on: April 12, 2015
28.3.15
A laparoscopic appendectomy in a 35 years old male had to be converted to open operation when the appendix could not be found. At open operation, the appendix could be palpated, buried in the retroperitoneum retrocecally. Thereafter, it was removed retrogradely.
1.4.15
A difficult TEP repair of a right inguinal hernia. The thick big sac contained omentum, which had to be reduced from below and then the sac could be dissected free, and was ligated with vicryl.
4.4.15
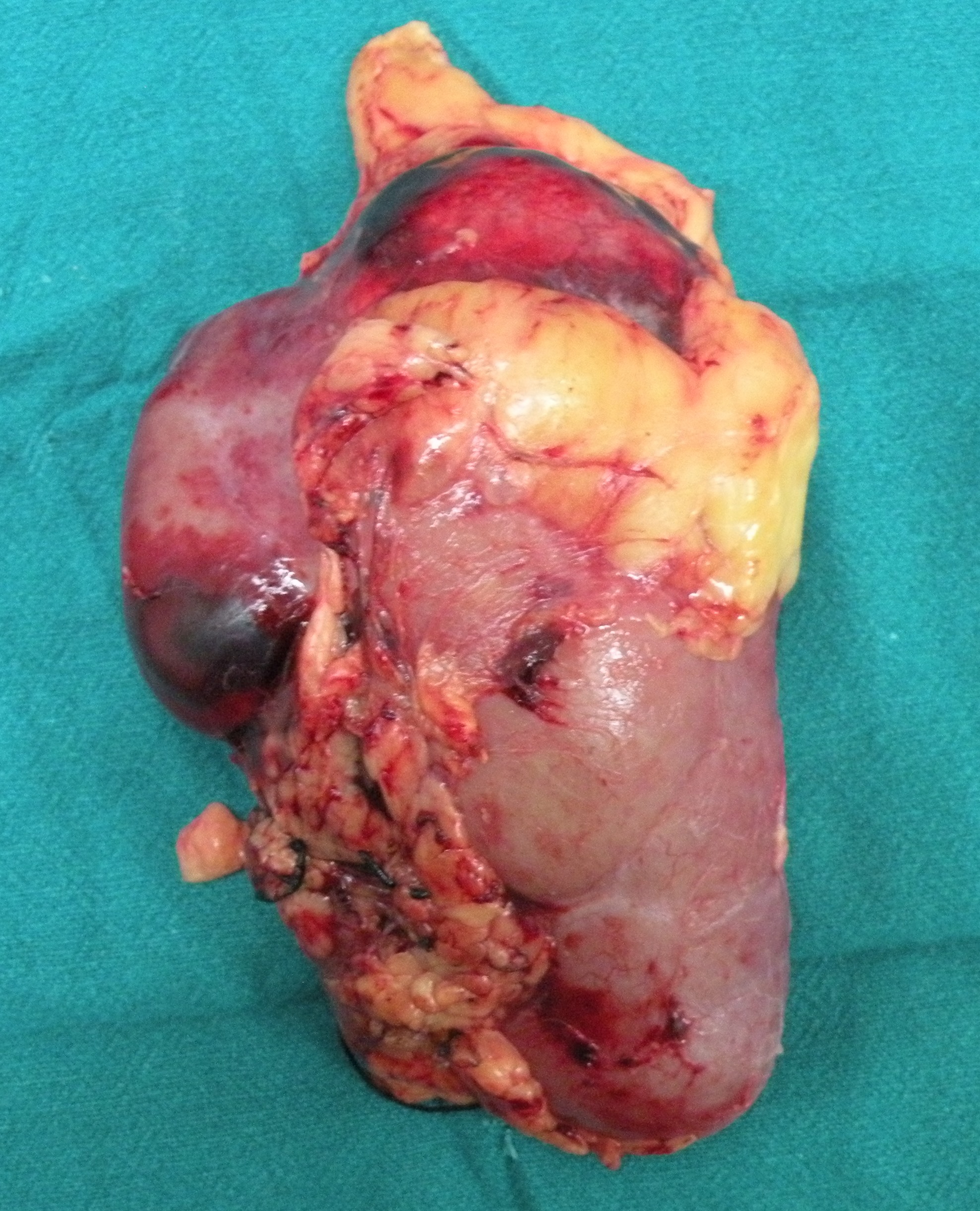
A testicular tumor in a young male (32 years old), with high level of tumor markers, was removed through inguinal approach.
.
5.4.15
Laparoscopic cholecystectomy (dr Grover’s daughter-in-law, herself a doctor), recorded by dr Grover’s camera (handycam).
10.4.15
Anderson-Hyne’s pyeloplasty for right sided hydronephrosis due to congenital UPJ obstruction, in a 22 years old female.
11.4.15
Laparotomy for intestinal obstruction of 7 days duration, not resolving on conservative treatment, in an 85-years old lady (mother-in-law of dr Darshan pal Sharma). There was an omental band causing the obstruction, this was divided. The patient needed ICU care postoperatively due to bad lungs (crepts bilateral).


Adrenal indicentaloma
Posted on: March 18, 2015
18.3.15 A frustrating experience with laparoscopic attempt at removal of a large (>6 cm) adrenal incidentaloma of the right adrenal gland in an obese 40 years old man (c/o dr sandhu, senior resident). Poor unhelpful liver retraction of a large pendulous liver by the absent-minded assistants who would rather injure the liver than retract it strongly upwards, poor camerawork by the other unhelpful assistant who would just fail to concentrate on his job, and poor anaesthesia by the junior residents who would just not accept that the patient needs good relaxation, led eventually to conversion to open procedure at which the tumour was easily removed. 
 the biopsy was reported as benign – myelolipoma.
the biopsy was reported as benign – myelolipoma.
Adhesive intestinal obstruction, a lap chole using harmonic scalpel, a twisted big fibroid misdiagnosed as appendicitis, and a pulsatile vessel seen in the floor of the Rouviere sulcus
Posted on: March 11, 2015
14.2.15
An elderly female (70 years old) admitted with intestinal obstruction (previous history of 2 caesarean sections) kept on conservative treatment but did not respond in about a week’s time. At laparotomy, a jumbled up mass of some 6 inches of ileum containing a tight stricture had to be excised, and an EEA made.


23 and 24.2.15
PG class on CRC and seminar on faecal fistula on consecutive days.
28.2.15
A lap chole for acute cholecystitis using Harmonic scalpel (for thesis) throughout the dissection, helped in saving time and blood loss. Also made the operation easy by reducing the smoke compared with cautery.
4.3.15
Bilateral TEP repair for inguinal herniae in 40 years old mess servant.
A planned appendicectomy in a 60 years old female actually turned out to be a big twisted fibroid revealed at diagnostic laparoscopy. Converted to open to remove the big fibroid, the pedicle of which had taken three turns.
11.3.15
Lap chole following pancreatitis. Turned out to be quite difficult with a big Hartmann pouch hanging much below the level of the Rouviere’s sulcus. The notable feature of the sulcus was a visible pulsating vessel in its floor.
A thyroid cancer, a few TEP hernia repairs and a few wrongly diagnosed cases
Posted on: February 7, 2015
27.11.14
TEP repair of right inguinal hernia performed on a 70-year-old man referred from Khanna by Dr Bhasin. Needed to have a urethral meatotomy and bladder catheterization also for narrow meatus associated with a glandular hypospadias.
1.12.14
TEP repair of right inguinal hernia in a young 20-year-old resulted in a pneumothorax and collapse of left lung. Kept in ICU for a few days after chest intubation for expansion of the lung.
10.12.14
A big sliding hernia (right inguinal) in a 60-year-old, contained cecum, appendix and omentum, repaired with a mesh.
29.12.14
MRM for a multicentric tumor in right breast in a 76-year-old lady (mother of dr Vinod, ex resident) from Sangrur.
Laparoscopic orchiectomy for undescended testis in a 20-year-old male.
TEP repair of bilateral inguinal herniae, 45-y-old male, worker in the hostel mess.
6.1.15
A very difficult open CBD exploration (55-year-old female) after a previous failed attempt at cholecystectomy at some civil hospital. Dense adhesions all around the shrunken gallbladder, eventually the GB and CBD were identified, a cholecystectomy was performed, a big stone found and removed from the bile duct and a T-tube inserted.
A wrongly diagnosed appendicitis (burst with diffuse peritonitis) in a very sick toxic patient (60-year-old female) actually turned out to be a caecal perforation due to a palpable tumour in the cecum. A right hemicolectomy was performed and the ileum and colon exteriorized after thorough peritoneal lavage. The patient stayed in ICU for 4 days and then recovered.
21.1.15
A hemorrhoidectomy (70-year-old female wit big prolapsed piles, mother of Dr Girish Sahni, ortho) performed with harmonic scalpel turned out to be neat and bloodless.
24.1.15
An anal fistula, diagnosed wrongly as a sinus only because its inner opening was not demonstrated clinically and even on a sinography and MRCP, was found to he a fistula, the whole tract of which was excised. The patient a government servant, 45-year-old male and a diabetic.
31.1.15
Two TEP repairs with harmonic scalpel very satisfactory and bloodless, one had a thin sac and the other a thick sac, both sacs ligated with an endo-loop and excised.
2.2.15
At lap chole, a RHD or the CHD was already found to be injured (small hole) by the diathermy hook before I reached the scene. Dissection completed by me and a drain left in the sub-hepatic space.
4.2.15
A difficult lap chole , started by dr Walia (A P), had to e completed by me.
5.2.15
An 11-year-old child (dr Jagga’s case), diagnosed wrongly with burst appendix (based on US report) actually turned out to have no appendix (agenesis) , but had some fluid in the pelvis, which was sampled for culture and microscopy.
7.2.15
A total thyroidectomy with lymphadenectomy in a 35-year-old-female for FNAC diagnosed papillary carcinoma (dr Usha Chhbra, HOD anatomy’s case). Strangely, biopsy was reported as Hashimoto’s thyroiditis!. 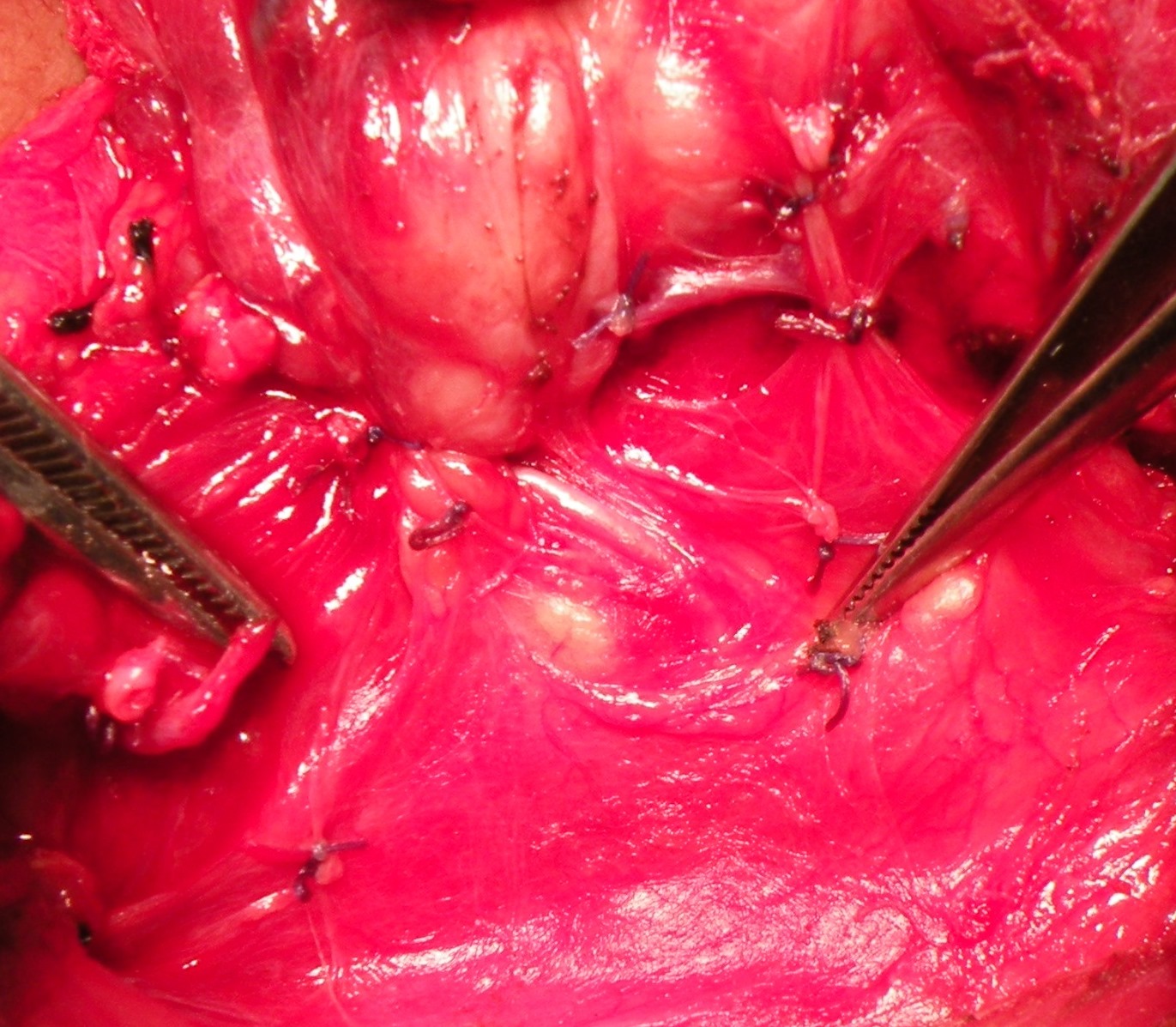



An adult intussusception, a TEP hernia repair converted to open repair and an anomalous Luschka’s duct identified after division
Posted on: November 20, 2014
10.11.14 An anomalous duct of Luschka was identified only after division, at a lap chole in a 55-years old female. The proximal end was sought in the liver bed and clipped (Dr GS Sandhu (senior resident)’s case).
13.11.14
A planned LIH repair by TEP approach had to be abandoned and converted to open hernia repair due to a hole in the peritoneum at the time of creation of space, and loss of space thereafter.
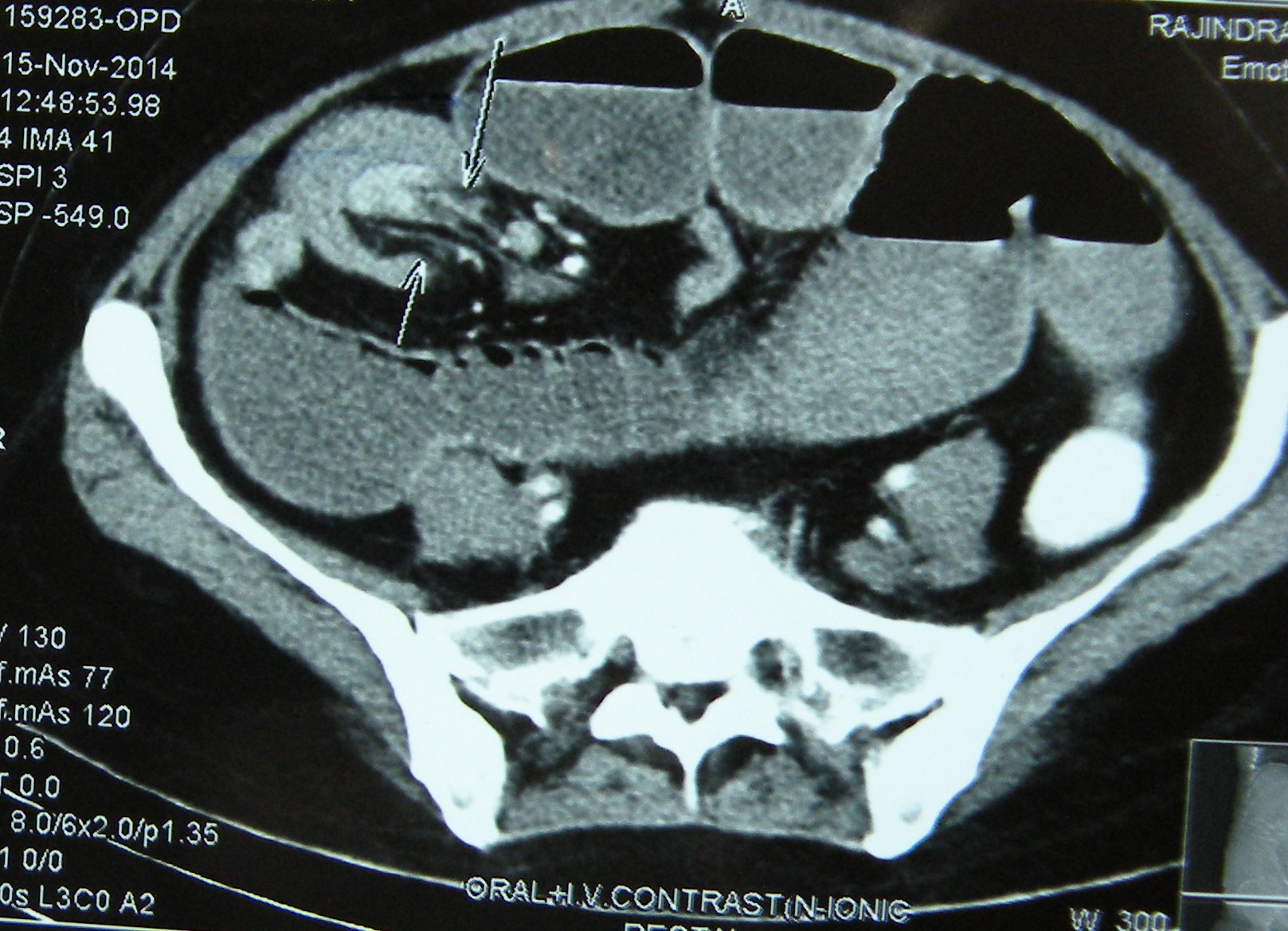
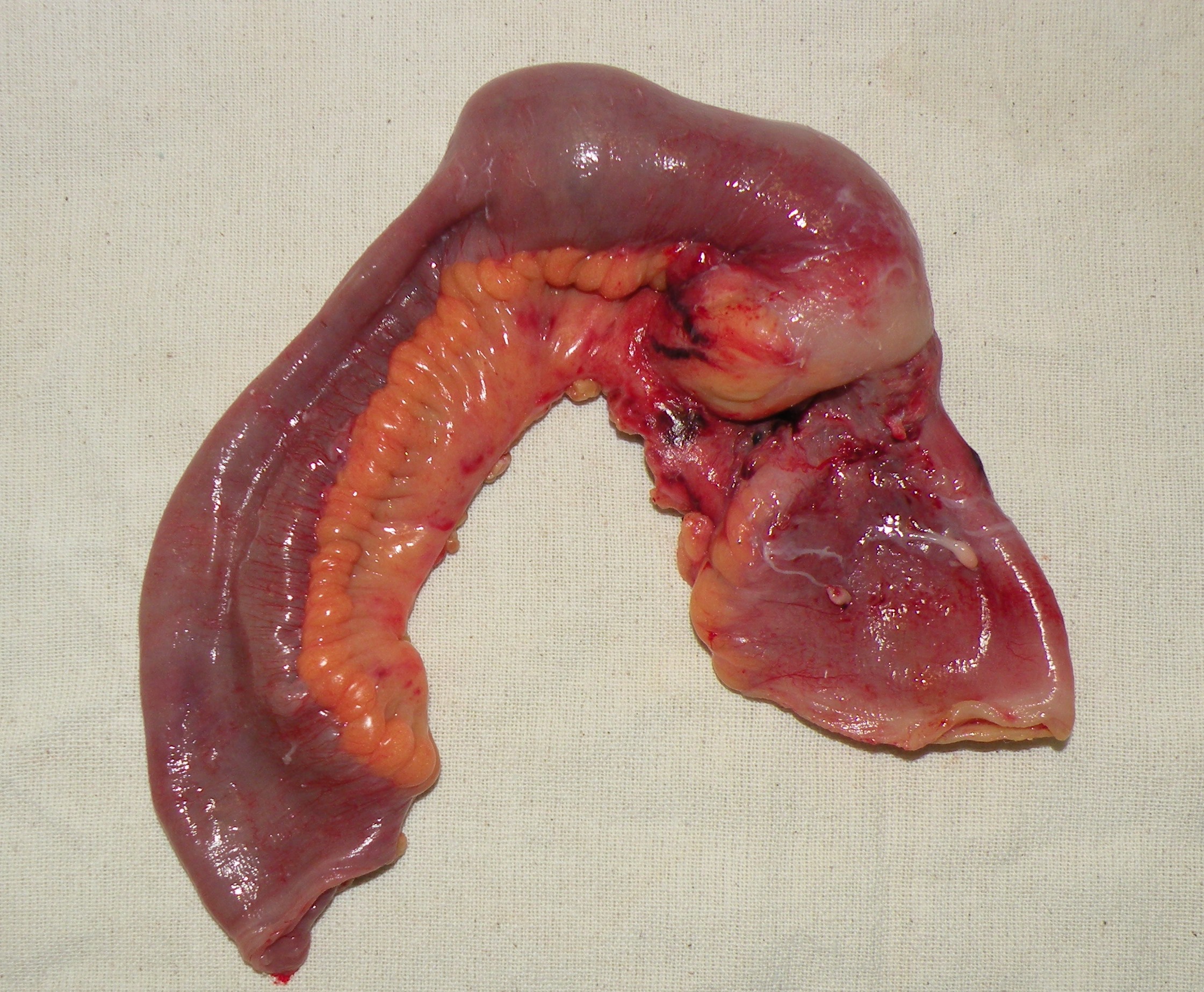
20.11.14 An adult intussusception, diagnosed on US and CT, in a 50-years old female, presenting with sub-acute intestinal obstruction of many weeks, was treated by resection of the segment of distal ileum bearing the intussusception. On cut section, it was found to contain a big pedunculated benign-looking tumour arising from the ileum. 

A Spigelian hernia, a meeting with Dr Robert Rutledge and some difficult lap choles etc.
Posted on: November 9, 2014
28.9.14
Attended a CME (by IMA) at Khanna and chaired a session on ‘mini gastric bypass’ by Dr Robert Rutledge.
6.10.14
Some difficult lap choles, in one of which the Rouviere’s sulcus showed a pulsating vessel in its base.

20.10.14
A relaparotomy for a mass in the right colon which had been deemed unresectable by the residents and a proximal ileostomy had been done. At operation, the mass was indeed found to be fixed to the posterior abdominal wall, encasing the ureter which was dissected clear. However, it remained a palliative resection. The ileostomy was taken down and an EEA (Ileocolic) performed. Biopsy was adenocarcinoma. To be referred for chemotherapy.
30.10.14
Incisional hernia at the medial end of a Kocher incision for open cholecystectomy. A 55 years old lady, known to Dr Didar Singh Walia (forensic medicine). Mesh placed in a the preperitoneal space.
3.11.14
A lap chole in a young (25 years old) male, who was admitted with acute cholecystitis. The gall bladder was thick-walled and showed patched of gangrene in the fundus. Difficult dissection of the triangle of Calot.
8.11.14
A Spigelian hernia in a hefty 40 years old patient, weighing over 90 kg. Presented like appendicitis with pain in the right lower quadrant. The CT however made the diagnosis. Through a lower midline laparotomy, the congested ileal loop trapped in the hernial sac was released from the neck of the sac. The sac was excised and a prolene suture repair, reinforced with a patch of mesh between the muscles and the peritoneum, performed.



Renal cell carcinoma
Posted on: September 19, 2014
7.9.14
A big renal cell carcinoma (more than 19 cm across) involving the superior pole of left kidney and adherent to spleen and tail of pancreas in a 35 years old female, excised through anterior approach. The pedicle slipped leading to considerable bleeding and panic. The bleeding was controlled with the help of a vascular clamp and sutures.

16 and 17 august
Attended a urology conference (north zone, urological association of india) along with dr sukhpreet and dr grover. Watched interesting surgeries: laparoscopic partial nephrectomy, laparoscopic radical prostatectomy, RIRS and mini-PCNL etc.
27.8.14
Assisted dr Vikram in a lap chole in which a stone (impacted in the neck of gallbladder and had eroded into the wall of the bile duct – Mirizzi syndrome) had caused transient jaundice last week although the LFTs were normal now. The dislodgment of the stone left a defect in the wall of the bile duct. This defect was covered with a flap of the wall of the gallbladder neck which had been left as a long stump after ligating the gallbladder neck. Bile leaked for 10 days through the drain, then dried up.
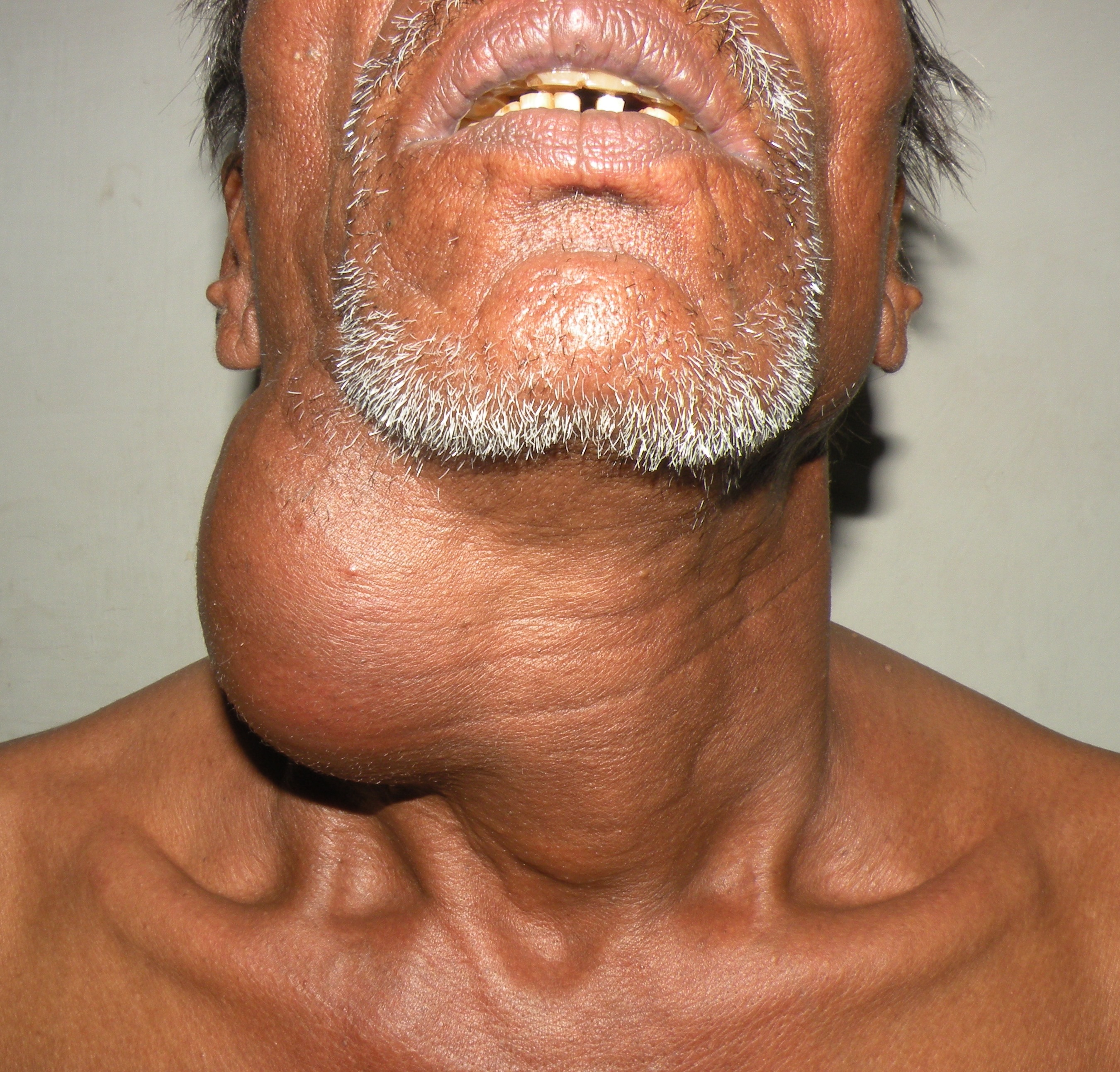
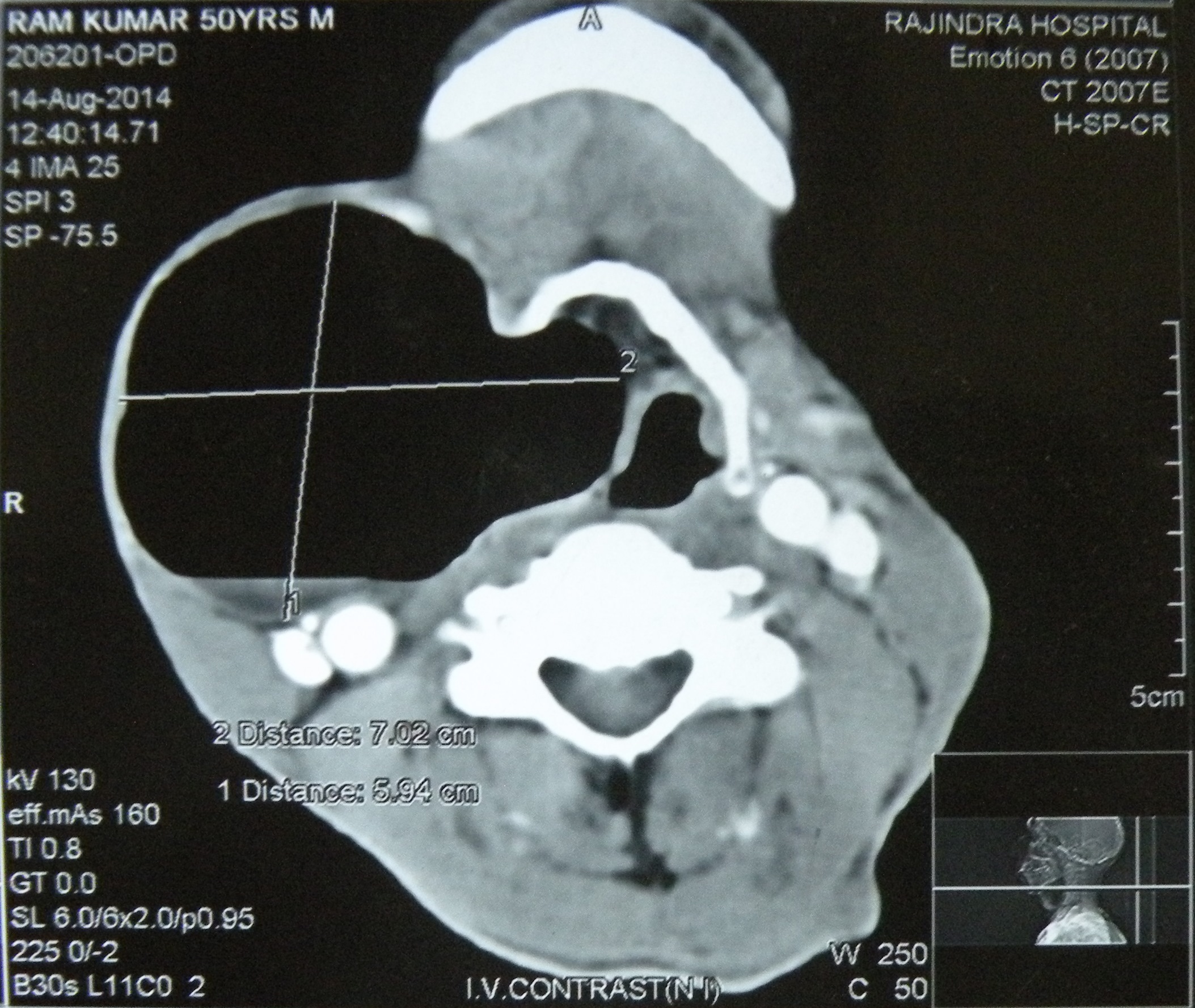
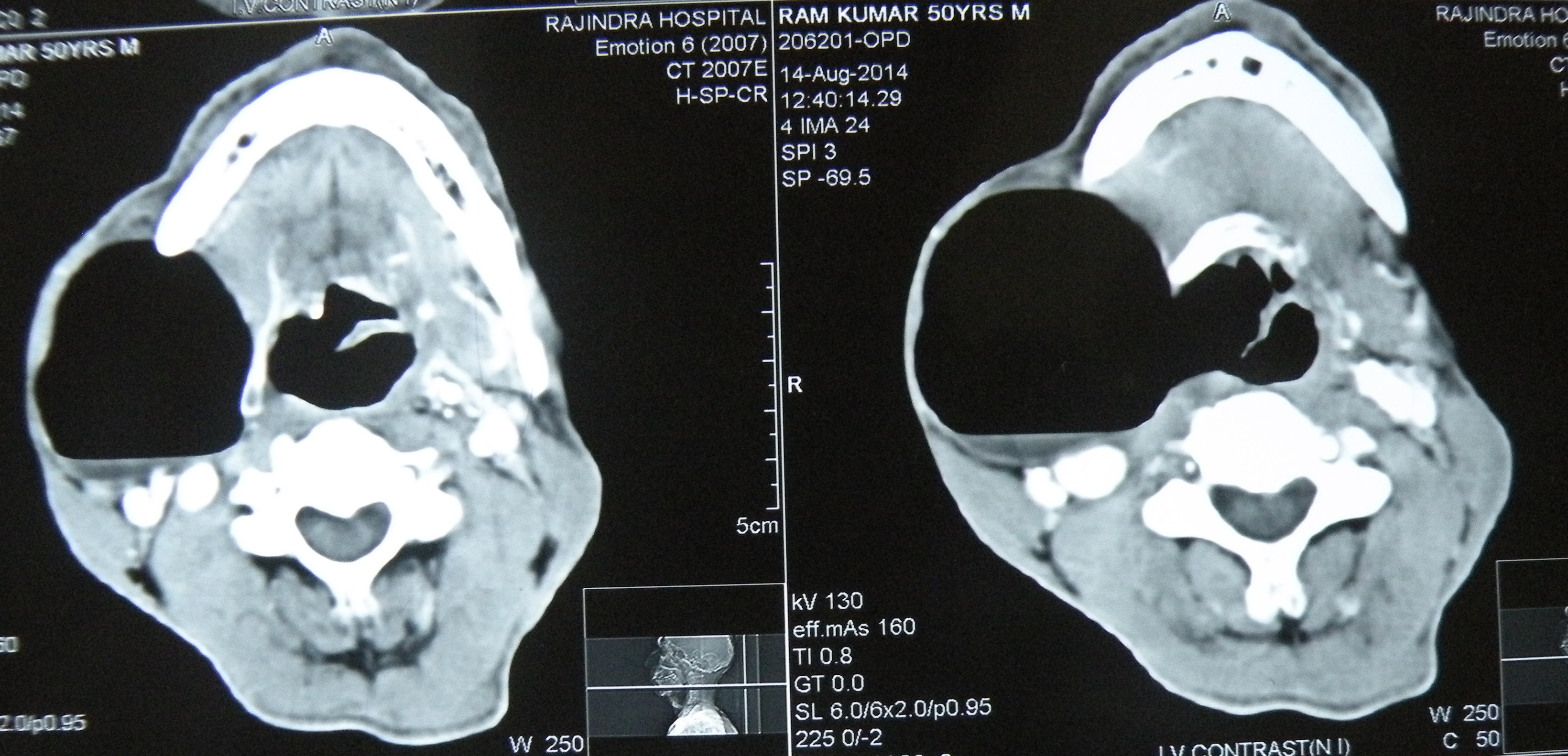
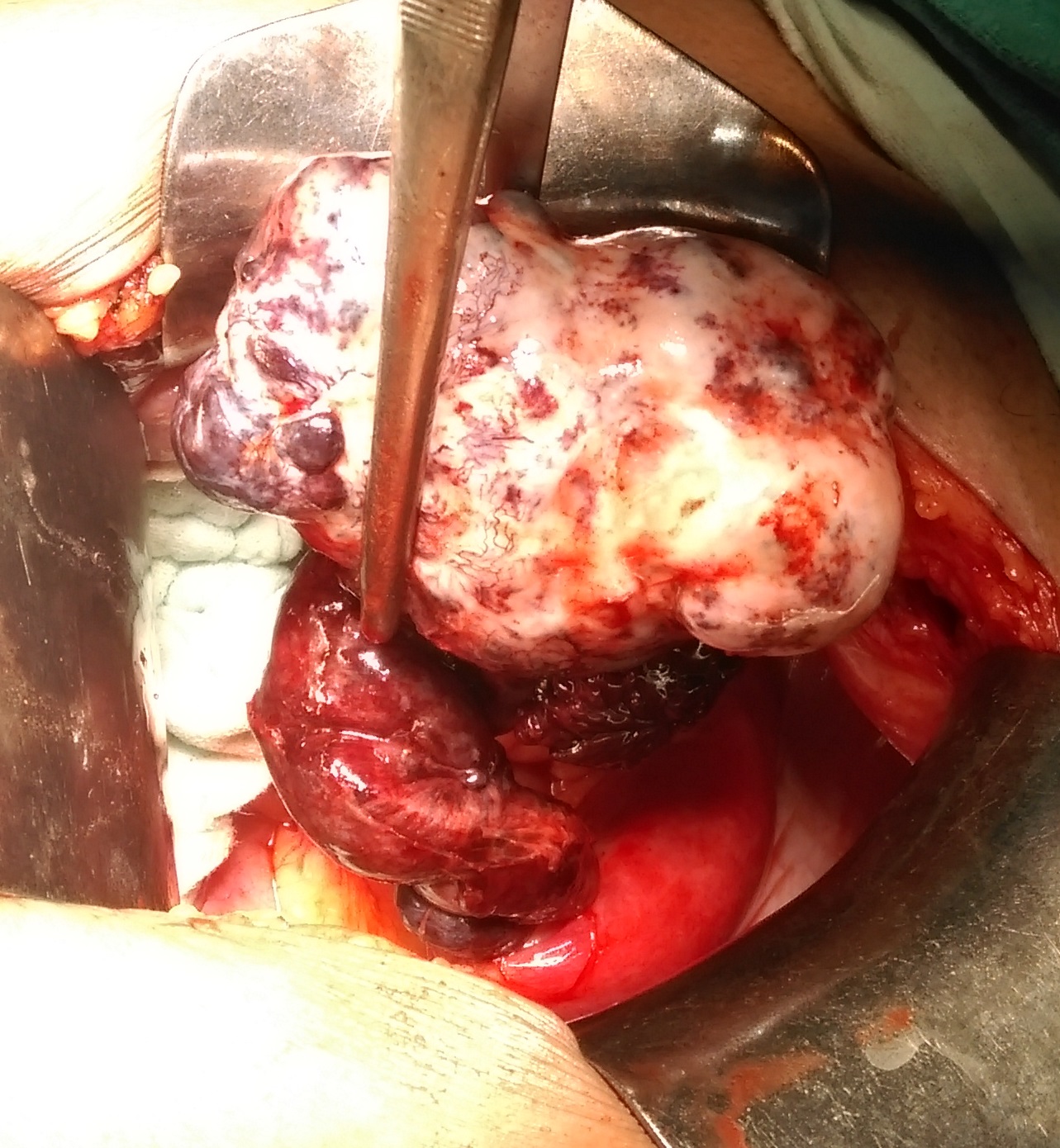
28.9.14
Repaired a large laryngocele for the first time in life!. Had never seen it actually before this one. An old man ( a chronic smoker) had been having a large swelling on the right side of the neck for a long time, and now had been experiencing some pain and hoarseness of voice. ENT examination revealed an internal component of the laryngocele too which had displaced the larynx to the left.