Author Archive
Roux-en-Y duodenojejunostomy for SMA syndrome, a stricture at the lower end of ureter, a bad anal fistula, Harmonic lap choles, two wrong diagnoses, and a subtotal colectomy
Posted on: August 14, 2014
15.6.14
A wrongly diagnosed stone at lower end of ureter was found to have no stone, and actually a stricture for which the ureter was reimplanted into the bladder after excising the stricture. Dr Jagga’s case, a 7 years old male child.
8.7.14
A very bad chronic anal fistula with extensive suppuration and fibrosis all around the track, all of which had to be excised leaving a deep defect in the ischiorectal fossa, that eventually healed satisfactorily. Patient reported to be very happy! Had been suffering for long and had a couple of surgical attempts earlier.
28.7.14
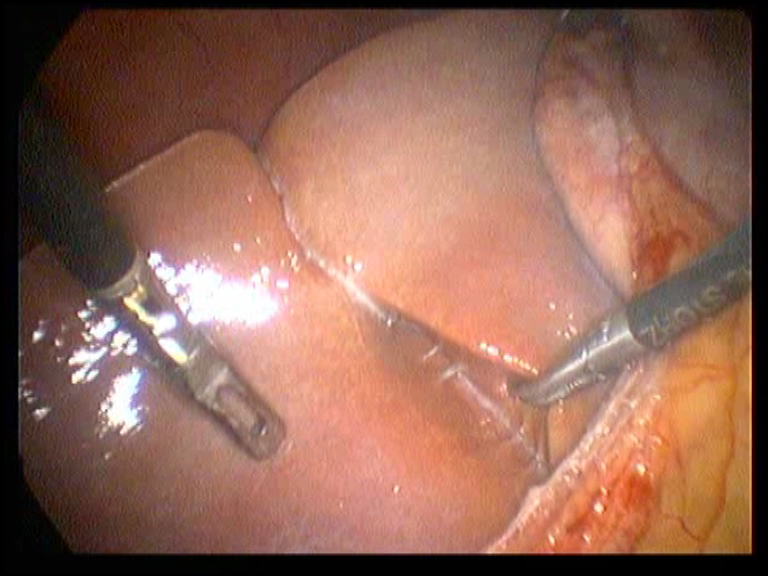
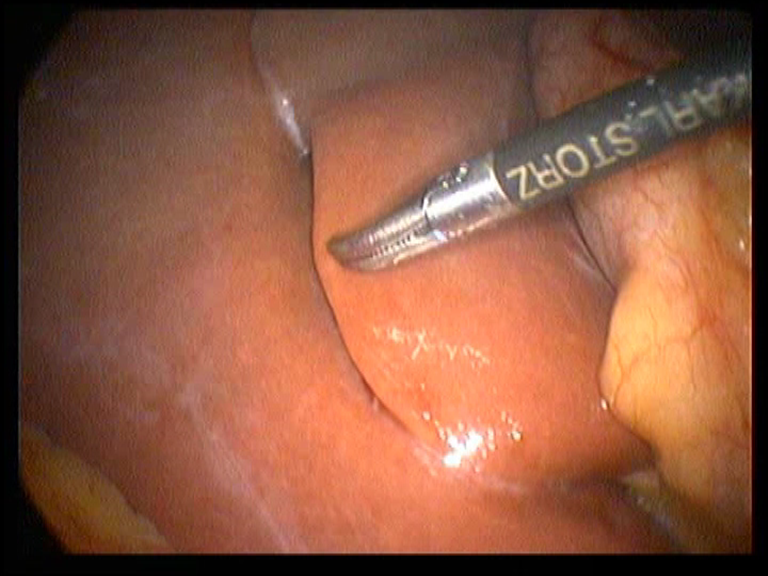
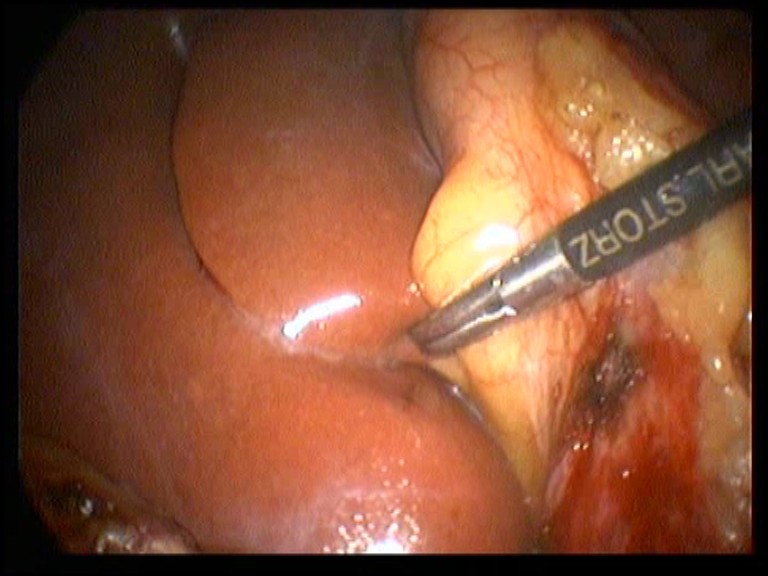
2 lap choles done with Harmonic scalpel, neat and clipless division of the cystic duct performed for the thesis work of a resident.
31.7.14
A disappointing day.
A presumably easy lap chole for chronic cholecystitis turned out to have what looked like extensive intraperitoneal deposits and some ascites. Transverse colon was found to be densely adherent with the anterior abdominal wall making entry of subxiphoid port dangerous. The ascitic fluid was sampled and omentum biopsied. Cholecystectomy was deemed not possible. The biopsy report surprising came out to be tuberculosis!.
A young female (35 years old, HIV positive), had a mobile big intraperitoneal mass, reported on CT as ovarian (CA 125 also elevated). At operation the clinically mobile mass was found to be a mass in the greater omentum between the stomach and colon, but had a more extensive fixed retroperitoneal component posteriorly. Only a biopsy only was possible; and this was reported as sarcoma.
11.8.14
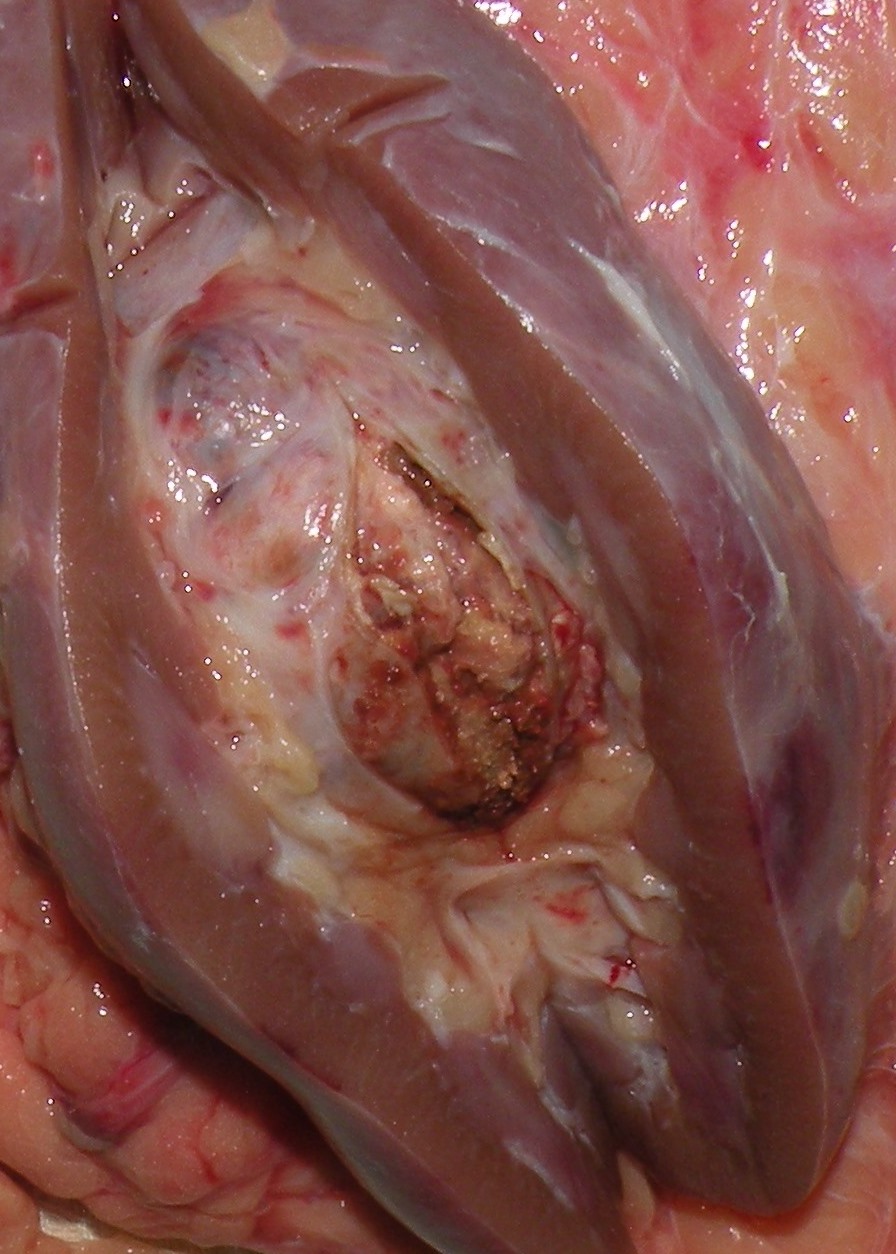
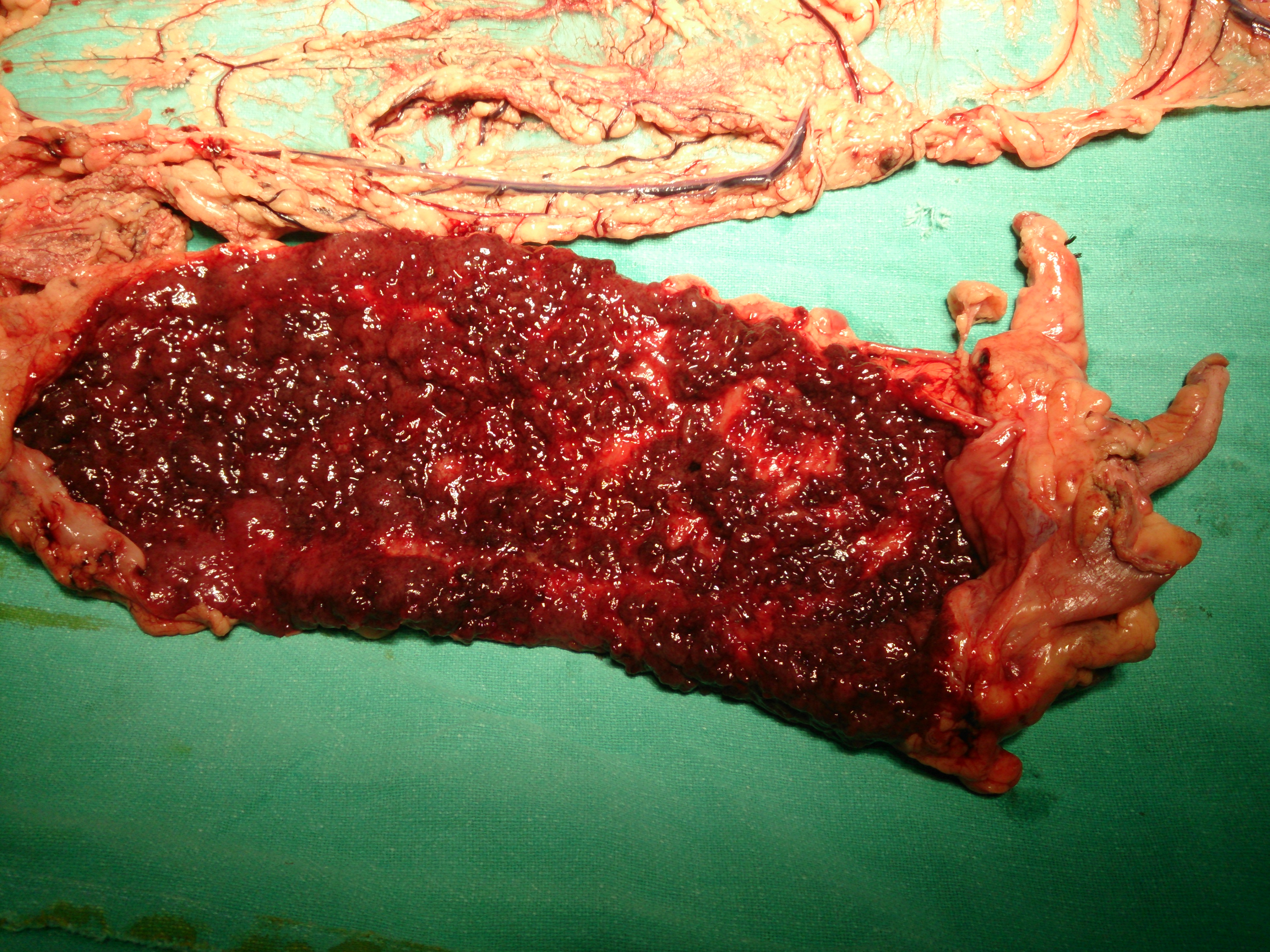
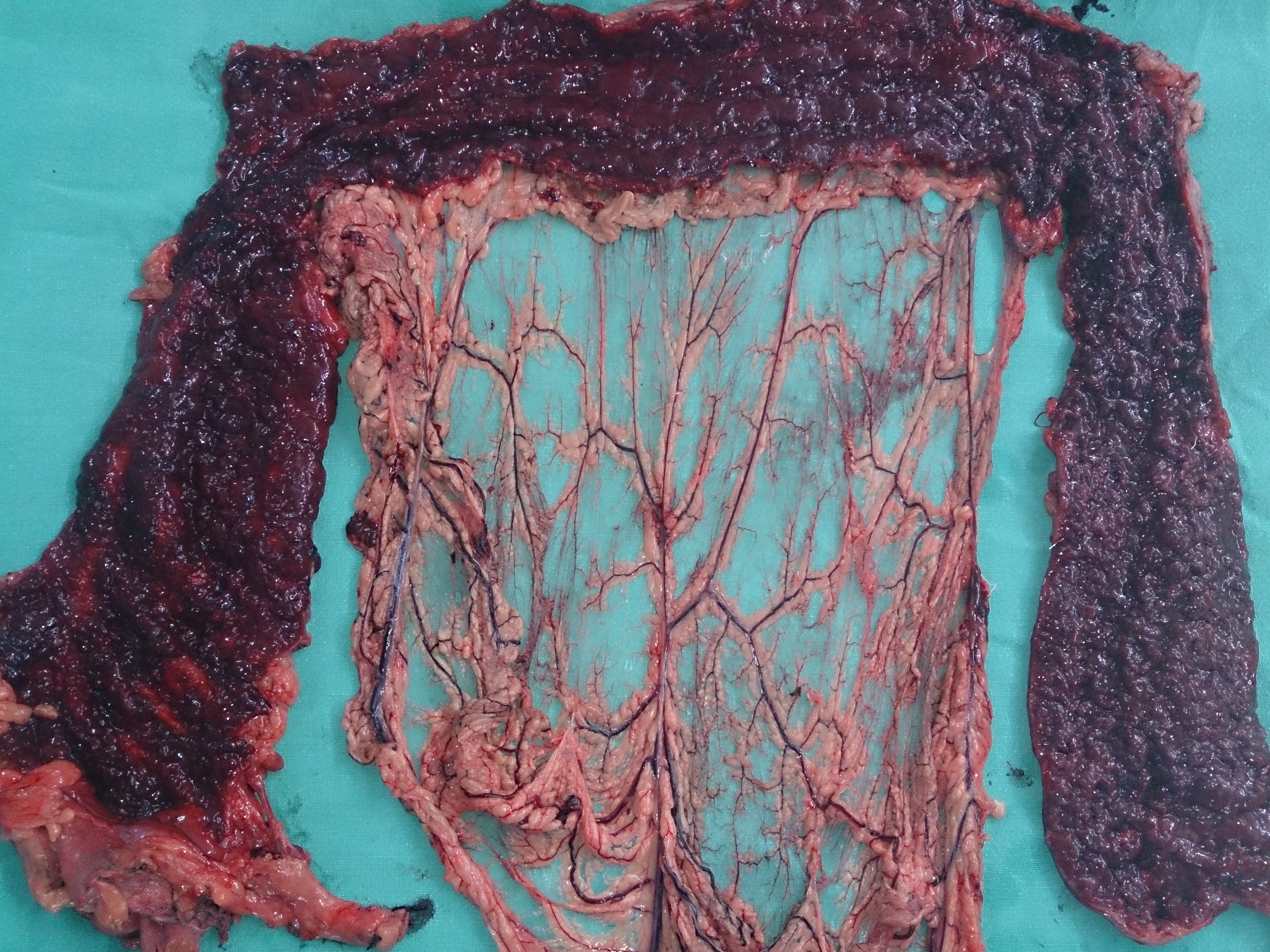
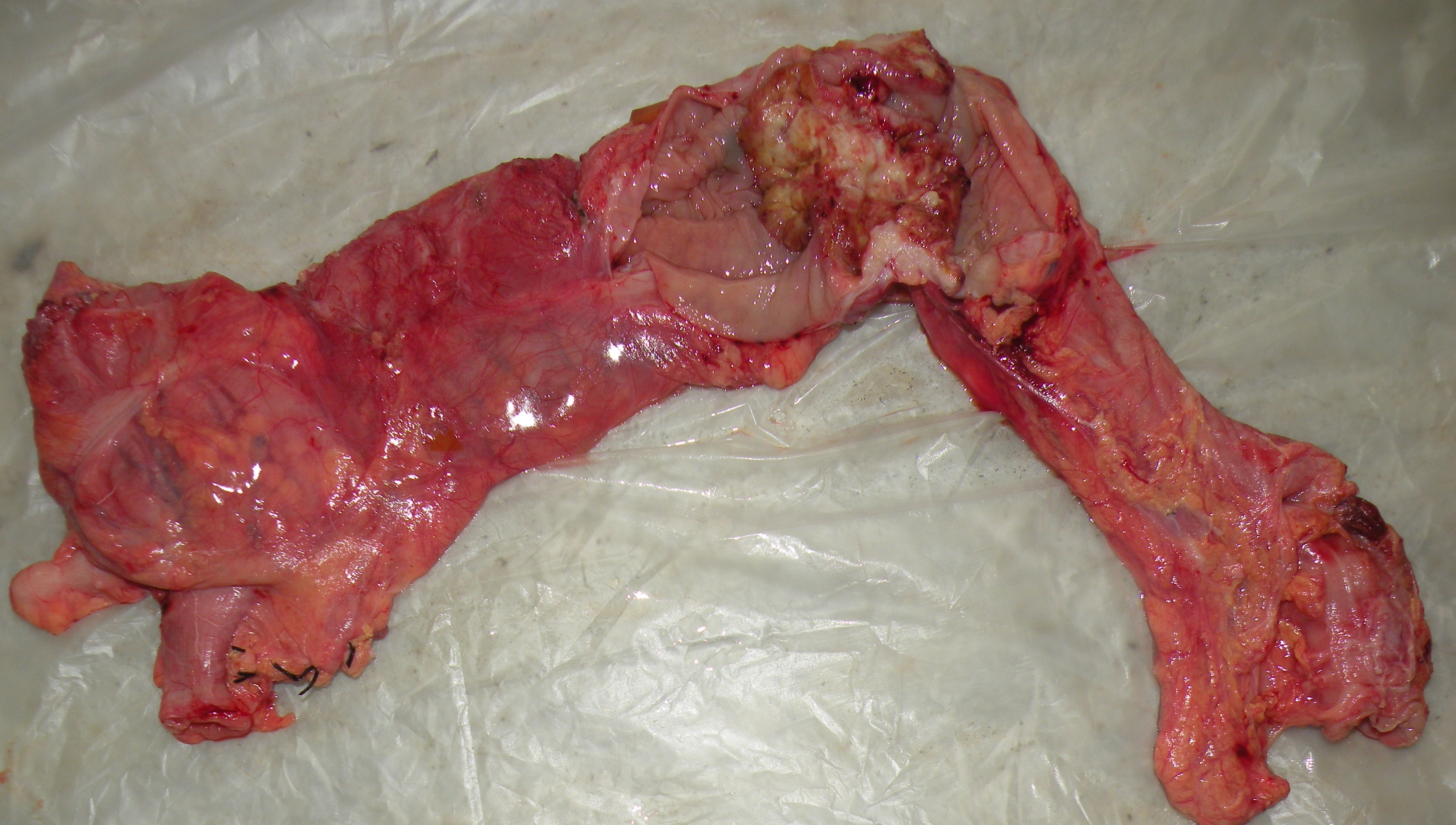
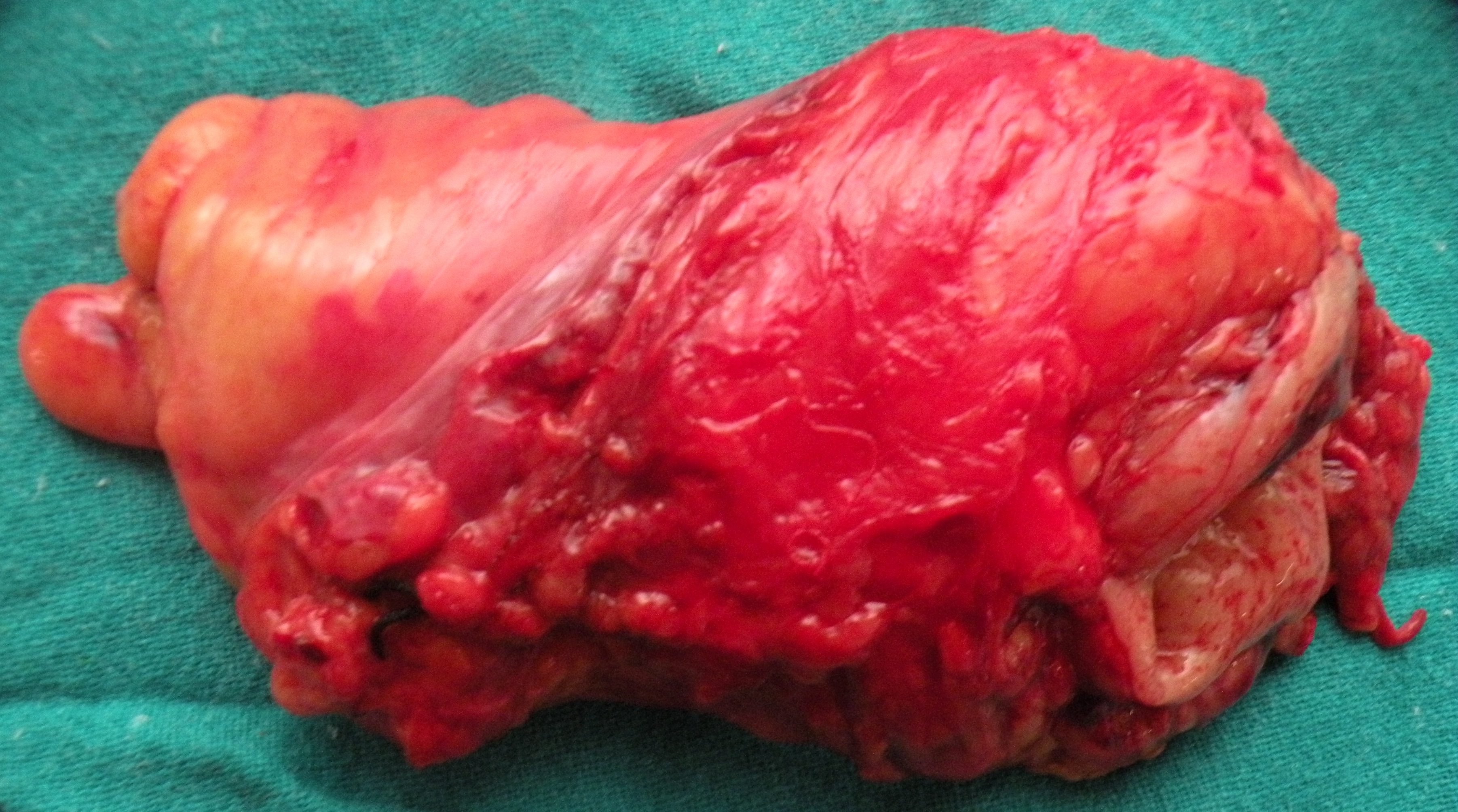
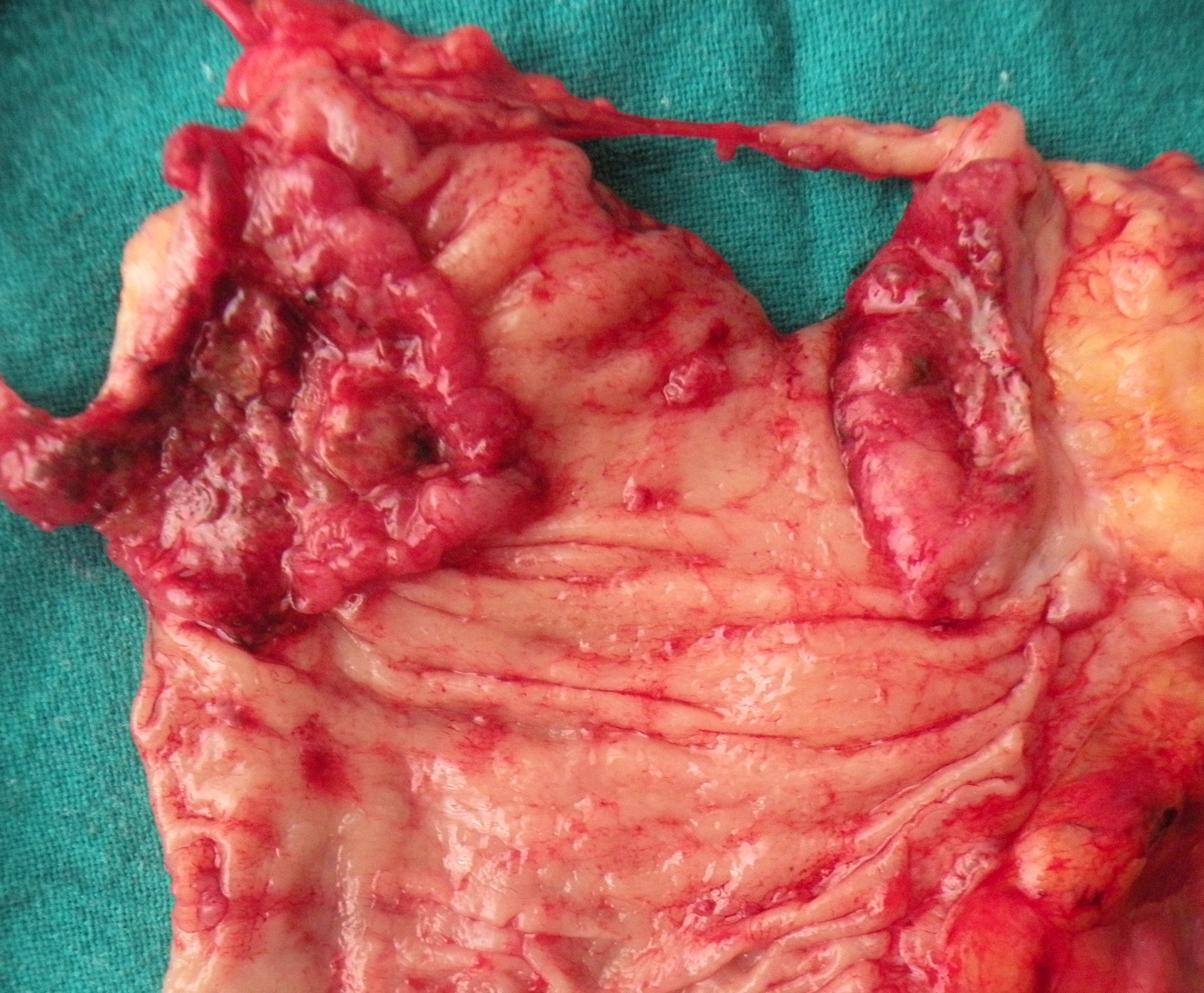
Subtotal colectomy and ileostomy for severe ulcerative colitis (pancolitis). Young (25 years old) patient, with fulminant ulcerative colitis, which had had remissions earlier, but now had actually become more severe, with the patient having developed abdominal pain, as well as increase in the number of bloody stools (now more than 10 per day). Referred from medical ward for surgery.

14.8.14
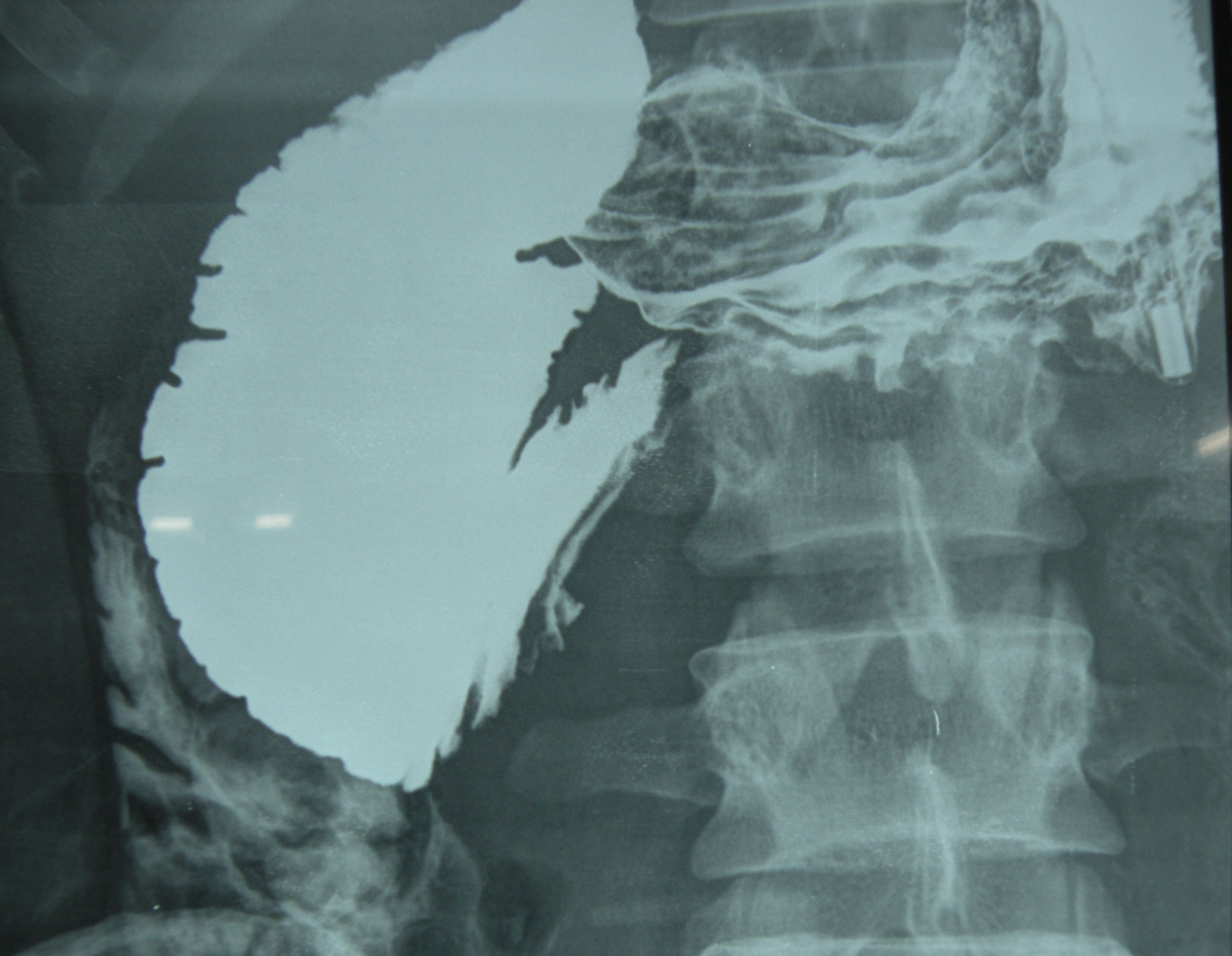
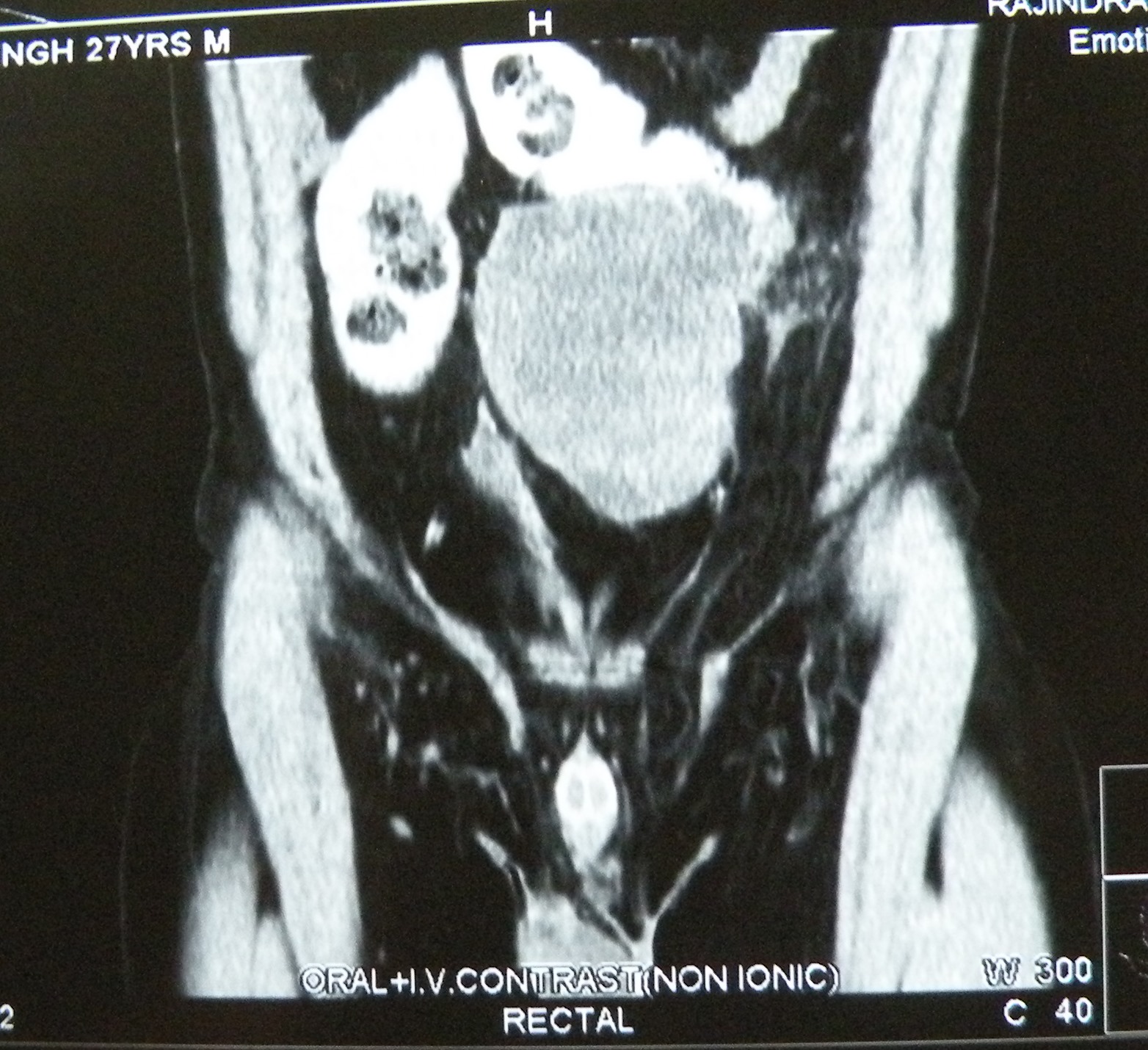
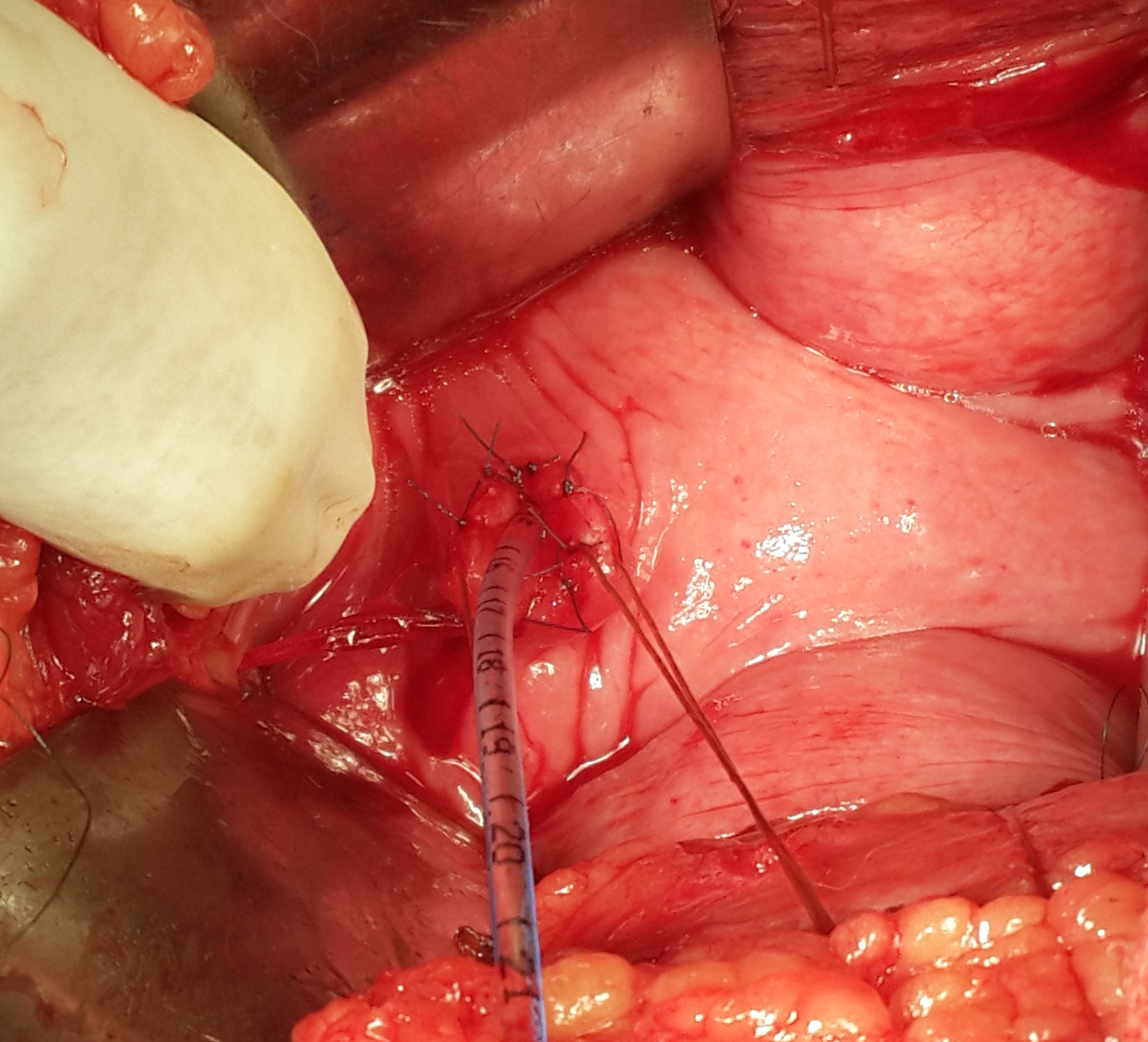
Roux-en-Y duodenojenunostomy for SMA syndrome. The young patient (27 years old) had undergone an appendicectomy (perhaps a wrong diagnosis) at Samana about two weeks back, but continued to have abdominal pain and vomiting. Barium study revealed a dilated duodenum up to the third part.
The angle between the aorta and SMA was 15 degrees on CT angiography.

At operation, after mobilizing the duodenum, the patient was found to have omental adhesions in the right lower abdomen ( at appendicectomy site). These were lysed. Interestingly, the upper small bowel had herniated through a hole created between the loops of proximal jejunum which were densely adherent to the posterior abdominal wall.
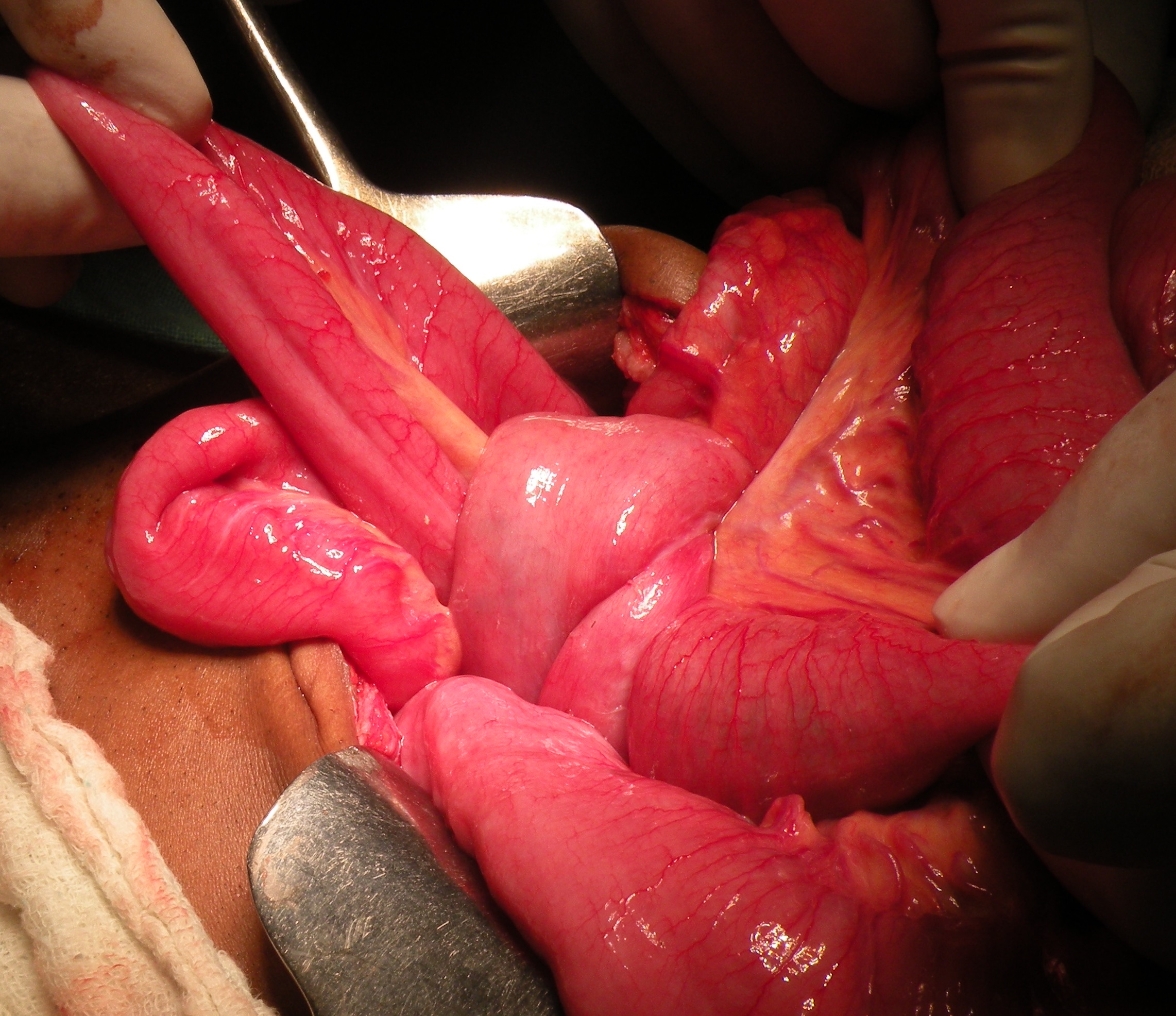
These adhesions were divided, and the jejunal loops released, only to find some stricturing in a loop at the site of adhesions. This upper jejunal loop was excised to remove the strictures and a Roux-en-Y DJ was performed for cure of the SMA syndrome as well.
- In: general | operations
- Leave a Comment
8.5.14
An anomalous bile duct encountered at lap chole and clipped.
Incidentally, the Rouviere’s sulcus in this patient was jus a slit.

12.5.14
An old man (65 years old) reported to have a mass in the caecum (on CT scan) turned out, at operation, to have an appendix abscess with gangrene of the wall of the caecum, for which resection of the caecum and an end-to-end leocolic anastomosis had to be done.
19.5.14
A difficult lap chole in an obese 55 years old hypertensive lady (dr SK Jindal’s relative). The gallbladder was almost entirely intrahepatic, thick-walled and packed with large stones. the stones were removed first to empty the gallbladder and helping to grasp the thick walls of the gallbladder. Since the Calot’s triangle was obliterated, the gallbladder neck was ligated with vicryl, and the gallbladder removed in pieces since it would not otherwise come out through the 10 mm port. The patient remained in ICU for one day, but recovered very well.
6,7,8 june, 2014
Attended the free medical camp at Baru Sahib. Performed 12 open cholecystectomies (laparoscopic equipment not available), 2 PUH repairs, one hydrocelectomy, one cystolithotomy, and 2 inguinal hernia repairs, besides excision of a couple of lipomas.
Mesenteric fibromatosis, vesicovaginal fistula and big sebaceous cysts on the scalp
Posted on: May 1, 2014
- In: conferences | operations
- 1 Comment
10.3.14 An incisional hernia gone wrong. A young man with incisional hernia (following laparotomy for ileal perforation) had a mesh repair of the same. However, postoperatively, the suction drain started discharging darkish brown content. At relaparotomy, a loop of small bowel had been caught in the suture meant to fix the mesh. Ileostomy was carried out along with peritoneal lavage.
20.3.14 An attempted TEP hernia repair had to be converted to open repair due to poor creation of space and poor muscle relaxation.
24.3.14 A nephrectomy (anterior approach) for renal cell cancer of the left kidney in an obese 60 years old lady, c/o Dr Walia our assistant professor.
31.3.14 A difficult lap chole in a 50 year old female admitted for acute cholecystitis 3 days back. Surgery very difficult due to thick-walled empyema. The gallbladder was removed piecemeal, after ligating its neck with vicryl.
3.4.14 An open prostatectomy after a long time in a 70 years old man, with the prostate more than 120 grams in weight.
4 and 5 April, 2014 Attended the AMASI conference in Simla.
7.4.14 An easy TEP hernia repair in a direct right inguinal hernia.
10.4.14 A lap chole for acute cholecystitis turned out to be very easy!
12.4.14 Presented a case of ‘mesenteric fibromatosis’ in the clinical meeting held in the medical education cell of the college. An 11 years old child was shifted from paediatrics ward, with a history of fever but was found to be having a big palpable mass in the right iliac fossa. A CT scan showed a 10 cm big well-defined mass in the peritoneal cavity. At operation, the mass was found to be arising from the mesentery of the distal ileum. The mass and the adherent loop of ileum were resected. Biopsy revealed an aggressive fibromatosis of the mesentery.



Mesenteric fibromatosis presenting as a diagnostic dilemma: a rare differential diagnosis of right iliac fossa mass in an eleven year old-a rare case report.Mahajan A1, Singh M1, Varma A1, Sandhu GS1, Singh M1, Nagori R1.
18.4.14 A VVF (poor 45 years old lady) following an abdominal hysterectomy in UP, was repaired abdominally. The fistula was high in the fundus of the bladder.

1.5.14 Huge sebaceous cysts on the scalp removed painstakingly, taking more than 2 hours!.



published in:
Journal of Clinical and Diagnostic Research. 2015 Nov, Vol-9(11): PJ01-PJ02
6.3.14
A 27 yeas old male, HCV positive, presented with a mass (15 cm across) in the left lower abdomen, and found to have an undescended testis on examination. AFP and HCG grossly elevated. At exploration, the big tumour was found to be adherent to the sigmoid colon, which had to be resected along with the tumour.

An arteriovenous malformation on the forehead in a 22 years old man, previously incompletely excised in Haryana, excised again after ligating the feeding superficial temporal and other small vessels.


A breast lump in a 60 years old female, negative on FNAC and Core needle biopsy, excised widely. Cut section typically scirrhous.
Jejunal duplication and stricture, a pyelolithotomy, and a parotidectomy
Posted on: February 17, 2014
An unusual presentation for a small tubular duplication and stricture of jejunum causing obstruction in a 60 years old lady. The jejunal segment was excised and an EEA performed.
23.1.14
A difficult lap chole in 50 years old male (Bhupinder singh from kheri) with a thick-walled mucocele, removed piecemeal.
3.2.14
A pilonidal sinus (recurred after 7 years), in a 25 years old male (s/o Dr Avinash Gupta ortho), excised and sutured. close
5.2.14
Pyelolithotomy for a big staghorn stone left kidney, and a small impacted stone in lower calyx, removed through nephrolithotomy. 40 years old male with the other kidney nonfunctioning due to ureteric stone, drained through a nephrostomy tube, for later possible nephrectomy.
6.2.14
laparoscopic repair of a portsite hernia (through the umbilical port of lap chole 3 years back), repaired with proceed mesh.
11.2.14
MCI inspection in the college. The hospital turned 60 years old, the staff celebrated by cutting a birth day cake and having photos with the medical superintendent dr Sharda.
17.2.14
Superficial parotidectomy for a 4 cm mixed parotid tumour in a 30 years old female, investigated in PGI.
 13.1.14
13.1.14
Transverse colon cancer, an ectopic pregnancy and a strange looking Rouviere sulcus
Posted on: January 4, 2014
19.12.13
MRM for an a breast cancer with open excision biopsy done at Rajpura civil hospital, no record available.
An extended right hemicolectomy for a transverse colon cancer in a 55 years old male. The patient had an interesting history of left colectomy with ileostomy (closed later) in Columbia Asia hospital about 3 months back, and now reporting with features of colonic obstruction and endoscopically diagnosed colon cancer again, this time in the right colon. An extended right colectomy was carried out; however, the whole left colon seemed to be intact and there was no sign of left colonic resection.

20.12.13
A right tubal ectopic pregnancy had ruptured through leaving a small hole in the tube. The hole was loosely closed with 4-0 vicryl.
26.12.13
A strange looking Rouviere’s sulcus seen at lap chole.
A low rectal cancer resection, an ovarian cyst wrongly diagnosed, a stone impacted in a ureterocele, some difficutl lap choles and an open cholecystectomy
Posted on: December 16, 2013
28.11.13
a A mesenteric cyst (diagnosed clinically and on CT) turned out to be big ovarian cyst. easily removed at laparotomy.
An impacted stone in a ureterocele, removed through open cystostomy and meatotomy.
30.11.13
A difficult lap chole, thick-walled gallbladder adherent to live bed which bled furiously, controlled with packing.
16.12.13
A rectal cancer (low) resected and a stapled anastomosis low in the rectum performed.

Posted on: November 19, 2013
18.11.13
Anal cancer – Abdominoperineal resection in a young (30 years old) male patient for anal cancer, previously treated by chemoradiation. Specimen on cut section showed only a tight stricture like a dense scar, hardly admitting an artery forceps.

28.10.13
Laparotomy for intestinal obstruction due to strictures diagnosed on laparoscopy on 24.10.13. Resection of about 2 feet of midileum bearing the strictures, followed by EEA performed.
31.10.13
SILS (single incision lap surgery) performed for the first time appendicectomy in a young female. Difficult due to parallel instruments.
7.11.13 to 11.11.13
Attended a conference (ICS-IS) at Lucknow along with drs jagbir and sukhpreet.
19.11.13 A total laparoscopic hysterectomy using Harmonic and en-Seal (Dr Mohi’s case) performed in gynaecology department.
Anal cancer resected after chemoradiation, and a laparotomy for ileal strictures
40 years old male, poor emaciated addict (bhukki) with repeated attacks of subacute intestinal obstruction. At laparoscopy, some adhesions in right iliac fossa, but the real cause of SAIO was multiple strictures in the small bowel about 50 cm proximal to the ileocaecal junction. Some fluid in the pelvis, was sampled for lab studies, especially for tuberculosis.


24.10.13
Radical nephrectomy for RCC
Posted on: October 21, 2013
21.10.13
Radical left nephrectomy for RCC in the middle pole of left kidney. Patient a 45 years old man (c/o worker at dr Sachdeva clinic). Had one episode of haematuria and CT showed the tumour. Anterior approach, removed with perinephric fat intact. No lymph nodes palpable.