3.3.11
A suspected urachal cyt just under the umbilicus in a 6 years old child excised.
7.3.11
a young 20 yearsl old female with a thyroid adenoma underwent a clean lobectomy but had hoarseness at followup a week later. The RLN had been clearly identified and preserved!.
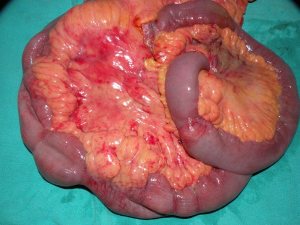
10.3.11
intestinal obstruction due to a band in 17 years old male, the badn divided.
12.3.11
emergency call for dr mohi’s patient who had a CS followed by hysterectomy yesterday, still in shock. The bleeders had to be ligated and then the patient repidly recovered.
15.3.11
Dr Bhatti from canada visited all colleagues here.
17.3.11
Lap chole converted after a long time.
21.3.11
TEP hernia repair for a direct hernia.
31.3.11
TEP for direct and small indirect inguinal hernia. c/o Dr KD singh, the principal.
2.4.11
india win the cricket world cup in finals defeating srilanka at mumbai.
17.2.11
Did a Bascom procedure for the first time for a recurred pilonidal sinus in a 25 y o male, relative of Kamlesh, the wonderful scrub nurse of old times!.
TEP repair of an obstructed left inguinal hernia, the big sac had reduced and had to be transected and endlooped. Used a large pore mesh.
24.2.11
Superficial parotidectomy in a young female for a 4 cm mixed parotid tumour, which turned out to be sitting beneath two branches of the facial nerve.

28.2.11
a presumably easy lap chole became very difficult. Young (25) y female with a previously acute attack was apparently normal now and taken up for lap chole. Turned out to have big empyema, adherent all around with omentum, colon and duodenum. Took 2 hours. Drained.
Misidentification of anatomy at lap chole, and giant condylomata acuminata
Posted on: February 15, 2011
- In: operations
- 2 Comments
13.11.2010
Misidentification of anatomy at lap chole caused panic. The lymphatics and fat with the cystic lymph node on top were identified as cystic artery and clipped and divided as such. Next the cystic artery was misidentified as cystic duct and divided as such after clipping. When the real cystic duct came into view, there was panic all around in view of the consideration that the main bile duct may already have been clipped and divided below having been misidentified as the cystic duct.
23.11.2010
Sternocleidomastoid tenotomy for severe torticollis in a 20 years old male.
25-28 nov. 2010
ICS conferenced attended in Pune.
30.11.2010
TEP using a light weight mesh. The sac had to be endlooped.
16-17 dec. 2010
ASI annual conference Delhi attended.
3.1.2011
Open cholecystectomy and CBD exploration after an unsuccessful attempt at endoscopic CBD clearance. Jaundiced patient. 55F. wife of Mr Jit Singh Virk. Sessile gall bladder, so the CBD stone could be milked up into gallbladder and removed without opening the CBD.
3.2.2011
Lap chole in an HIV positive 40-yr-old male, turned out to be very difficult. Dense adhesions and almost obliterated Calot’s triangle. The cystic duct could not be defined, so the gallbladder neck was endlooped and ligated.
12.2.2011
OPD pictures of giant condylomata acuminata.


29-31 october
National conference of National Academy of Medical Sciences held in the college auditorium. Delivered a lecture ‘biopsy tools and techniques as diagnostic modalities’ in the CME on breast cancer. Also chaired a session in the evening programme of the CME. The convocation was held on 30th when the fellows were awarded fellowships by the Governor of Punjab. The conference ended on 31st with some orations.
2.11.10
An adult intussusception reduced and limited ileocolic resection done. A 65 years old emaciated man with history of subacute intestinal obstruction and a palpable mass. US and CT suggested a colocolic intussusception. At operation, actually ileocolic intussusecption was found. This could be easily reduced, to reveal a small benign looking tumour. Limited ileocolic resection done with ileocolic EEA.


adult intussusception
Shinda’s marriage
Posted on: October 16, 2010
14.10.10
Attended at Chandigarh (sector 39 community centre) the pre-marriage ceremony (shagan) for the marriage of Surinder Pal Singh s/o Avtar Singh. Returned to Patiala in the evening in time to attend the award distribution ceremony for CBSE students who have secured admissions in professional colleges. Binu got her prize there.
15.10.10
Attended the marriage of Shindu at Samrat marriage palace, Samana. Anand karaj ceremony at Dhanthal gurdwara.
Abdominal cocoon, Breast ADH turned out to be IDC, SELSICON in Patiala, lap chole for retained GB stump, and a unique trichobezoar of matchsticks. shifted to wordpress from spaces.
Posted on: October 13, 2010
30.8.10
Ginu’s counselling (2nd) at faridkot bfuhs, gets Bathinda medical college. At last!
4 and 5.9.10
SELSICON annual national conference in our college, essentially a workshop. Interesting diverse cases of endoscopic surgery shown, including urological and gynaecologic and a 6-hour laparoscopic total proctocolectomy and IPAA.
7.9.10
Breast lump (60F) excised for FNA report of ADH. Later had to do a complete MRM for infiltrating carcinoma with positive lymph nodes.
14.9.10
A recurred high intersphincteric fistula excised.
21.9.10
Laparotomy for an abdominal mass in 35M with a mass and intestinal obstruction. Turned out to be an abdominal cocoon. The dense fibrotic cocoon excised and intestines freed. A short segment of ileum had to be excised.
2.10.10
A bezoar of matchsticks removed from the stomach of a young male child 5 years old!

5.10.10
Lap chole for removing a retained stump of gall bladder after earlier lap chole a few months back at Barnala had left a part ( the neck ) of the gall bladder.
10.10.10
GJ for GOO 35F with a diffuse thickening of wall of distal stomach extending up to D2 which being adherent to CBD was not excised, just bypassed.
12.10.10
Two unexpectedly difficult lap choles, both young (30-35) females, both had sessile gall bladder, both had to have fundus first dissection and the neck ligated with vicryl.



- In: operations
- 2 Comments




- In: operations
- 2 Comments




{kind=link}