- In: operations
- 2 Comments
10.8.10
A direct right inguinal hernia in a 62 years old male (himself a doctor, an ENT specialist) repaired (Lichtenstein). Husband of dr Marwaha, retired professor of gynaecology.
A breast lump, an antibioma with thick walls and thick pus in it excised. A 25 years old from Nabha, with history of swelling in the breast for more than 2 months, treated with antibiotics. Besides the thick walled big abscess cavity which was excised, there were areas of tiny abscesses around the main abscess arising out of dilated ducts – duct ectasia. These were opened up too.

An external angular dermoid excised under general anaesthesia.



- In: operations
- 2 Comments
5.8.10
One of the most difficult lap choles so far, worth remembering. A 40 years old man had been admitted two weeks before with acute cholecystitis, treated conservatively and recovered to be sent home. However, he was admitted again as he felt he had never been really free from pain. Ultrasound revealed distended gallbladder and pericholecystic fluid. LFTs within normal range. At lap chole, dense omental adhesions had to be removed diligently before the gall bladder became visible. A grasp at the fundus tore the gall bladder to reveal thick pus which was aspirated, and along with this came out a cast of a fibrinous wall of the abscess. Slow dissection led to the big Hartmann pouch the grasping of which was impossible due to the big stone stuck in it. This was opened up, the stone retrieved, broken into pieces to remove it piecemeal, and then only the neck of the gall bladder became clear. Further dissection of the area was deemed dangerous, and the neck was ligated with vicryl 1 twice with extracoporeal knots. Thereafter, separating the wall of the gall bladder from the liver bed was another difficult task, so some of the wall was left behind with the liver, and cauterised. Removal of the big thickwalled gallbladder was not possible in one piece, so it was divided in steps into 4 pieces, each one being removed separately. The whole procedure took nearly 4 hours, but in the end was a satisfying one. Next day the patient was smiling but the surgeon aching all over.
6.8.10
Anothe difficult lap chole, but not like yesterday’s. Male patient again.
AndersonHynes pyelopasty in a young (25) female, big hydronephrotic right kidney, with 29% function on DTPA scan.
A perianal fistula, starting from under the urethra with three openings and ending near the anal verge blindly. All tracks excised.
23.6.10
A laparotomy for dense ileal adhesions stuck in pelvis following TAH 10 days back. Lysis of adhesions, however, did not work and had to be reexplored to do REEA a few days later.
25.6.10
GOMCO 75 batch meeting at dr Zora singh’s place Chandigarh.
26.6.10
TEP reapir for RIH
6.7.10
saw dr grover recovering after CABG at fortis, mohali
9.7.10
TLH : The urinary bladder got injured, repaired.
13.7.10
35 years old female with a big hydatid cyst posterior right liver. Partial cystectomy and omentoplasty after excision of cyst walls.
15.7.10
A big left parotid swelling, difficult parotidectomy, facial nerve in the tumour, sacrificed. Biopsy reported as lymphoma!
20.7.10
Orchidopexy for undescended testis located at the internal ring. 10 years old child from Patran. IE vessels divided to gain length.
30.7.10
A paratidectomy, mixed parotid tumour, facial nerve nicely displayed and protected.
3.8.10
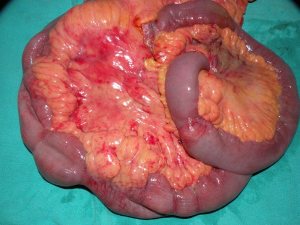
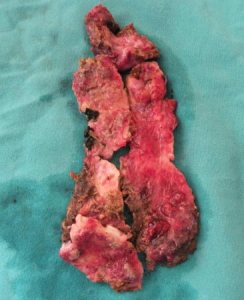
A planned right hemicolectomy became extensive resection of distal ileum and right colon. A 35 years old female admitted with a mass in right iliac fossa not resolving. CT showed a long tubular stricture in the whole of right colon, The mass regresses somewhat with conservative treatment. A barium enema showed a tight stricture reportedly in the right colon. At exploration, multiple strictures in the terminal ileum and some palpable thickening in the right colon, all of which was excised.



VVF repair and summer vacation
Posted on: June 20, 2010
18.5.10
50F with a right thigh swelling, twice recurred and now causing excruciating pain. Previous biopsy fibrous histiocytoma. Now again excised, but with wide (2 cm) margins. Skin closed under tension. Wound gaped after 7 days.
21.5.10
1. Young female (16 Kammo’s daughter). Two fibroadenomas apparently looking like one, excised under GA.
2. a big preauricular swelling (possibly dermoid) on right side in a 10 year old female child, excised under GA.
25.5.10
1. 50 year old obese female with varicose veins right leg. Trendelenburg + stripping + multiple phlebectomies.
2. VVF repair in a poor 60 year old lady who had the fistula for 15 years following a hysterectomy. Abdominal repair after splitting the bladder anteriorly. Fistula rather low down and between the two ureteric orifices which were identified and protected.
28.5.10
3 lap choles one after the other. The first two were easy. The third, Alka Rani (c/o Dr Suman from Phagwara), 50 F, hypertensive and diabetic, had a thick walled empyema. 200 ml thick pus aspirated. Difficult dissection in Calot’s triangle. Had fever postop for some days. Then gradually settled.
1.6.10 to 7.7.10
Summer vacation
6.6.10PMT test for binu and ginu at faridkot. binu got 17 rank and ginu 531.
MRM left breast for a big tumour (looked like cystosarcoma phyllodes, bosselated). Just one or two lymph nodes in the axilla.

19.6.10
Went to delhi with binu and Dr Jagga for binu’s CBSE counseling. Binu selected Patiala medical college. Returned late in the evening to Patiala.
20.4.10
Lap chole in a very obese (>120 kg) 35 years old female. Difficult due to fat in Calot’s triangle. Had to be kept in anaesthesia recovery for a very long time due to respiratory problems.
23.4.10
Varicose veins leg 35 M – Trendelenburgh, stripping to knee and multiple phlebectomies.
27.4.10
Thyroid lobectomy for recurred thyroid cyst after aspiration. 50F.
4.5.10
Extended right hemicolectomy 55 M from Dhanaula, with h/o anaemia, occult blood in stools positive and CT showing a mass in right colon. At operation, the cut section of specimen showed no real tumour inside but instead 3 strictures and multiple lymph nodes in mesocolon.Biopsy reported as eosinophilic colitis!!.


7.5.10
60M with h/o severe pain after every feed, CT showing dilated D1 and D2 and giving a diagnosis of SMA syndrome. Laparotomy – lot of ascitic fluid, missed on imaging!!. DJ flexure tightly fixed and scarred with nothing passing beyond into jejunum. No real tumour palpable. FNAC taken from dense retroperitoneal scar. GJ done. Cytology of ascitic fluid and FNAC came out to be negative for malignancy.!

11.5.10
TEP repair for bilateral inguinal herniae. 35M from Samana (dr Ashok Galib’s case)
12.5.10
Laparoscopic nephrectomy right non-functioning kidney.
Nephrectomy for RCC
Posted on: April 18, 2010
16.4.10
Nephrectomy for renal cell carcinoma lower pole right kidney. 35 M. BJP worker.Remains well on follow-up as of now (2013 april)

Some strange times
Posted on: April 11, 2010
- In: operations
- 3 Comments
26.3.10
Swelling left upper arm excised under GA. ?STS
28..3.10
Lap chole for acute cholecystitis, supposed to be routine. 35 F. US – polyp or sludge?
Actually a mass in fundus palpable at lap chole. Aspiration yielded dark blood!
Tense oedematous cholecystitis. Routine lap chole done. Biopsy adenocarcinoma.
30.3.10
Pilonidal sinus excised with primary closure. Did well. No recurrence.
31.3.10
Abdominal wall right flank incisional hernia repaired with mesh. 35F Sikh lady from Pakistan!!, with a history of RPM laparotomy (for what ?) with right flank drain in Pakistan. Hernia had developed at the drain site.
2.4.10
35M with previous h/o admission for appendix mass 3 months back. Hard mass still palpable. Ba enema reporting a filling defect. At right hemicolectomy, mass found to be posterior to cecum, but fixed to cecem and immobile. Could not be completely removed. Biopsy – inflammatory cells in one area behind the caecum – giant cells and fibroblasts. ?diagnosis.?bony. To be reassessed later.
5.4.10
To Simla to attend a second review committee to review the questions of MS/MD examination conducted by Simla university. Himachal high court had ordered to review the questions after students challenged some questions. The first review committee had only local faculty, so court asked for additional members from outside Himachal.
6.4.10
Thick walled empyema in 60 M. Lap chole.
7.4.10
Huge hydatid cyst superior half of right lobe of liver. 14 years old boy. Membranes removed intact and in toto. Huge cavity had to be capitonnaged and introflexed. Omentum not developed enough to bring into it. 

9.4.10
Had to atttend to summons from SP(D) (superintendent of police, detective) enquiring into complaint by relatives of a patient Manjit Kaur who had died of septic complications after left hemicolectomy for obstructing large splenic flexure adenocarcinoma; the patient had a leak and was reexplored 3 days later. Patient’s mother alleged that her kidneys had been removed!. What a change of times!
10.4.10
Imperforate hymen in 14 years old girl incised and dark blood (200 ml) drained.
11.4.10
TAH in a 12 years old girl!!. Mentally retarded with cerebral palsy and urinary and fecal incontinence. Mother’s insistence for the operation.
26.2.10
Lap chole in a 30 years old male (a surgeon himself, assistant professor, GSMedical college). Turned out to have a rather prominent accessory bile duct arising from the middle of the liver bed and draining directly into the gall bladder. After much deliberation and hesitation, this was doubly clipped and divided. Concerned at the prominent size of this duct though. Postoperative OK so far.



Right parotidectomy for chronic sialadenitis, causing pain and swelling during eating for last 10 years. 30 years old male. At operation, small pockets of pus in the parotid tissue. Dense fibrosis at places, making dissection of facial nerve branches difficult. Nonetheless all branches displayed and protected. Biopsy – chronic parotitis.
2.3.10
Easy male gall bladder in a 60 years old patient! Pleasant surprise.
Psoas abscess drained in patient with history of nepherectomy for RCC, followed by radiotherapy. Radiation induced myonecrosis?
3.2.10
TEP for bilateral inguinal herniae. Initial entry into preperitoneal space too superficial, nearly avusling the inferior epigastric vessels, which were coagulated eventually because of the continous bleeding.
17.3.10
Sacrocolpopexy for vault prolapse. Mesh strip buried under the peritoneum.
5.2.10
Haemangioma of neck. 45F with long standing swelling right neck, compressible but not expansile. Excised under GA.
Lap chole for huge empyema, 50 M. Aspirated before operation under US to emptiness. Later at operation, the huge thick walled gall bladder removed in 5 pieces.
6.2.10
TLH
12.2.10
A difficult lap chole for empyema. 45 M with empyema gall bladder, wanted early operation. Big stone from within the gall bladder removed after fragmentation.
16.2.10
TEP right indirect inguinal hernia. 25 M. the sac divided and endlooped. Poor light and leaking trocars!.
A huge swelling right neck in 25 M, pressing on trachea and shifting it to other side. bulging in floor of mouth. Excised under GA. contents like dermoid.



18,19,20 february
attended the annual conference of IAGES at Delhi..
21.2.10
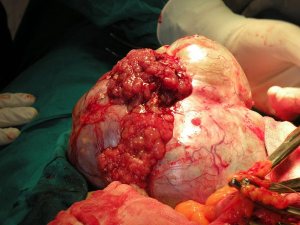
A huge fungated ovarian tumour, malignant, 45F. TAH bSOP and omentectomy. Clinically presumed to be benign in an otherwise very fit looking patient.


Re-exploration of rectopexy, etc
Posted on: January 28, 2010
30.12.09
Rectopexy done 10 days back re-explored for adhesive intestinal obstruction.Adhesions in pelvis lysed.
5.1.10
Infiltrating type of huge lipoma thigh excised. 55F patient of dr Mrs Hans
12.1.10
3 lap choles.
18.1.10
Big perinephric abscess drained. Dr Jagga’s case.
22.1.10 Nephrectomy for RCC right kidney. 65 M.


{kind=link}
{kind=link}