Archive for the ‘Uncategorized’ Category
Piecemeal removal of thickwalled difficult gallbladders offers many advantages
Posted on: August 28, 2021
25.7.21
A thick-walled gallbladder (with empyema and some gangrene in the fundus) removed in several pieces through the epigastric port without dilating or enlarging the port;

this has been the practice now for many years with me as it offers so many advantages:
- Grasping the gallbladder which has grossly thick and tough walls and which is often very big and tense (sometimes empyema or mucocele) is impossible; so opening the fundus first of all helps in suctioning the mucus or pus and decreasing the size of the gall bladder. The large stones are also removed from within and the empty gall bladder is washed clean. Now the grasper can easily hold the left or the right flap.
- The dissection if easy in the Calot’s area can now be attempted and completed if it is easy. If not stop;
- Most often in these cases the infundibulum too is grossly thick and can’t be held with the grasper; so, the incision from the fundus is extended down to the infundibulum and the anatomy re-evaluated after the grasper can hold the fundus flap on the lateral or medial side.
- Since the gallbladder is now of manageable size and can be held comfortably and the posterior wall of the gallbladder viewed closely with the camera zoomed in, dissection can begin above the Rouviere’s sulcus level on the medial side high up near the middle of the body of the gallbladder with a hook separating the peritoneum if possible and then if easy, the Calot’s triangle can be dissected as usual. If not easy, again stop.
- More often than not, however, the peritoneum is fused with the thick walls of the gallbladder and no plane of dissection is safely available.
- In such cases, starting again high up, a plane can be created with a hook through the thickened walls of the gall bladder and then with a suction cannula and a piece of gauze as dissecting tools one can often go safely behind the posterior wall or behind the mucosa of the posterior wall to emerge on the lateral side.
- This plane of dissection (mostly submucosal, under the mucosa or through the thick wall) is then extended down similarly with gauze and hydrodissection, occasionally assisted by the hook to cut away a tough adhesion, always under clear and close vision of the camera, down to the infundibulum or the neck of gallbladder whichever appears to be the narrowest part which is then simply ligated with no 1 vicryl using extracorporeal knot. Before doing this one must again confirm through the opened up gallbladder that no stone is left behind in the gallbladder.
- The GB is simply divided just above the knot and removed, but the posterior wall of the gallbladder is left behind, the mucosa to be cauterized just before closure.
- The 2 big flaps of the gallbladder still be need to be divided into more vertical strips to make it easier to remove those strips through the epigastric port one by one; thus ensuring:
- The procedure remains minimal access still, and
- The troublesome problems of gas leak and the heightened risk of incisional hernia through the dilated/enlarged port are avoided.
Moral and ethical issues in surgery – a ruptured tubal pregnancy; tubectomy or the other side – yes or no?
Posted on: August 5, 2021
4.8.21
A ruptured ectopic right tubal pregnancy wit hemoperitoneum in a 35 years old female was operated urgently due to severe pain in the RLQ; the US showing ectopic tubal pregnancy. A salpingectomy of the involved tube removing the products of conception in the tube was done along with peritoneal lavage. The lady repeatedly was talking under spinal anesthesia for tubectomy on the other side too. I asked the attending gynecologist dr Neena Sachdeva and she said the husband did not want it. So we did not do it. The next day during another surgery (LSCS), Dr Neena reported that the lady had married her present husband without telling him that she had had an earlier marriage and that she had 2 more children from that and so she did not want any more children and wanted a tubectomy on the other side too. She said it was right that we did didnt do the other tubectomy otherwise legal issues might arise later!
Branchial cyst
Posted on: July 20, 2021
8.7.21
A typical cystic swelling in lower left neck anterior to sternocleidomastoid in a 10 years old boy, typical of congenital branchial cleft cyst. Cytology supported the diagnosis (cholesterol crystals, squamous cells), but ultrasound suggested lipoma! Easily excised through a transverse incision. No associated sinus or fistula track.

24.6.21
Baljit Kaur 65 years old female

A detailed history of this patient’s journey towards several abdominal operations:
- Laparotomy (in PGI) in 1988 following enteric perforation of ileum resulting in peritonitis. The incision was long midline and vertical.
- 1992: the laparotomy was followed by an incisional hernia through that laparotomy incision; this was repaired possibly without a mesh in PGI again.
- 1996: an open cholecystectomy for gallstones was performed in Chandigarh government hospital sector 16, and they were told they also repaired through the same incision the incisional hernia which had recurred.
- 2000: An abdominal hysterectomy was performed (Shalley hospital) through the lower abdominal transverse (Pfannenstiel) incision.
- and 6. June/July 2021. The two surgeries given below starting with the incisional hernia first; and then
- a laparotomy for intestinal obstruction ending with resection of a big mass of matted small intestine which had been causing obstruction.
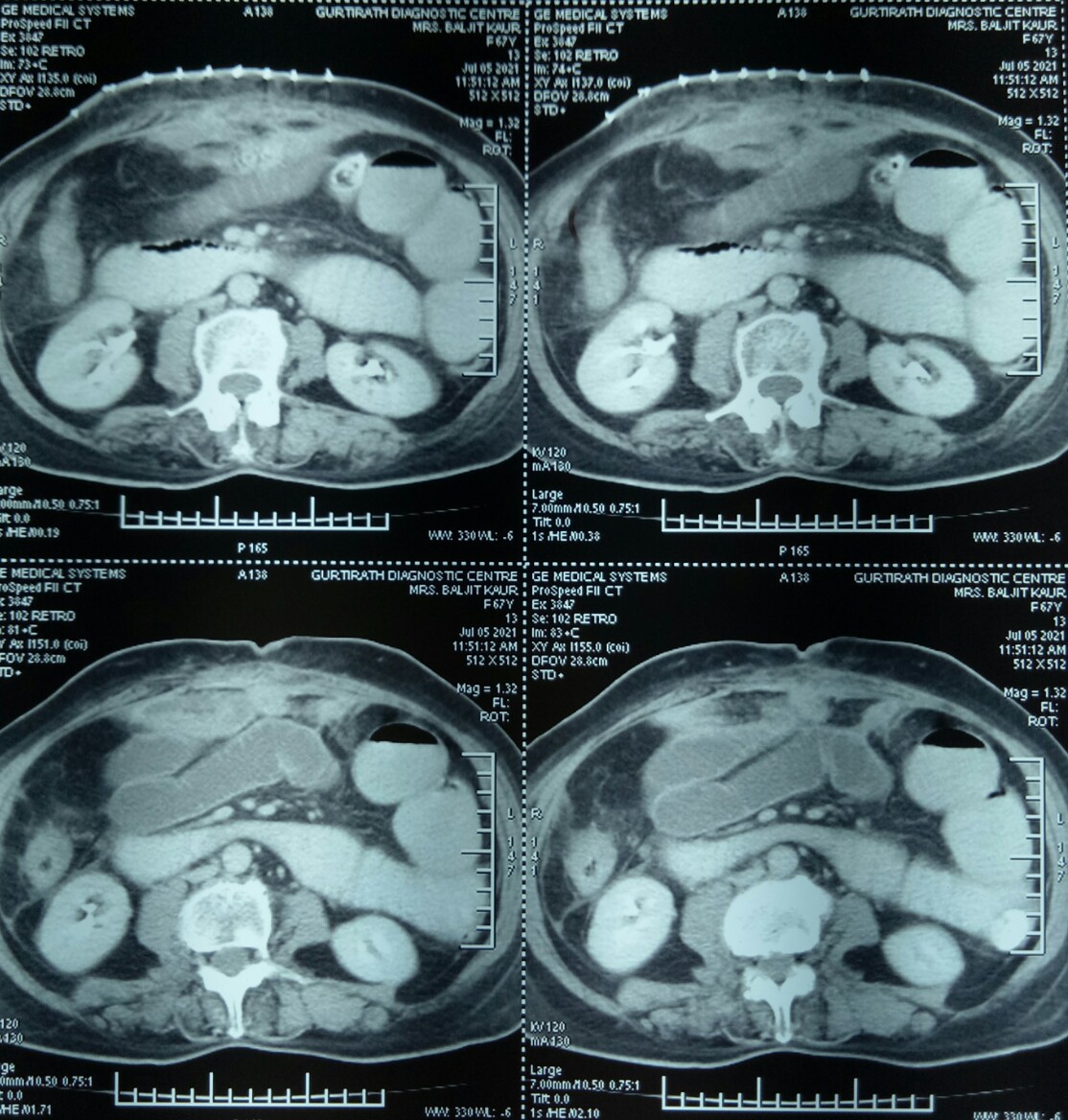
An incisional hernia (that had recurred perhaps for the third time) in the right upper part of the abdomen repaired in a 65 years old female. Because of the history of multiple operations earlier, a CT scan was performed and showed a defect in the anterior abdominal wall with a loop of intestine protruding.

Presuming it to be a routine case of an incisional hernia where the intestinal loop will be reduced back into the peritoneal cavity and the defect repaired, we started happily. But it turned out to be a nightmare when the loops of intestine just could not be separated from the edges of hernial defect, and it was discovered that some of these loops of small bowel were trapped in the prolene sutures used for the hernia repair earlier.
Diligently and slowly (taking nearly 3 hours, so as not to end up in a perforation) the intestinal loops were freed as much as possible through this incision and the hernia defect then defined after repositing the loops into the peritoneal cavity. The defect was then repaired with prolene sutures and a prolene mesh.
Postoperatively the patient seemed to be making good recovery for the first 3-4 days but then started having distension and vomiting, suggesting intestinal obstruction which did not respond to conservative treatment.
CT scans confirmed grossly dilated small bowel loops in the pelvis and left flank and one jejunal loop high in the centre, besides showing a mass of dense adhesions just under the staple line of the hernia surgery.

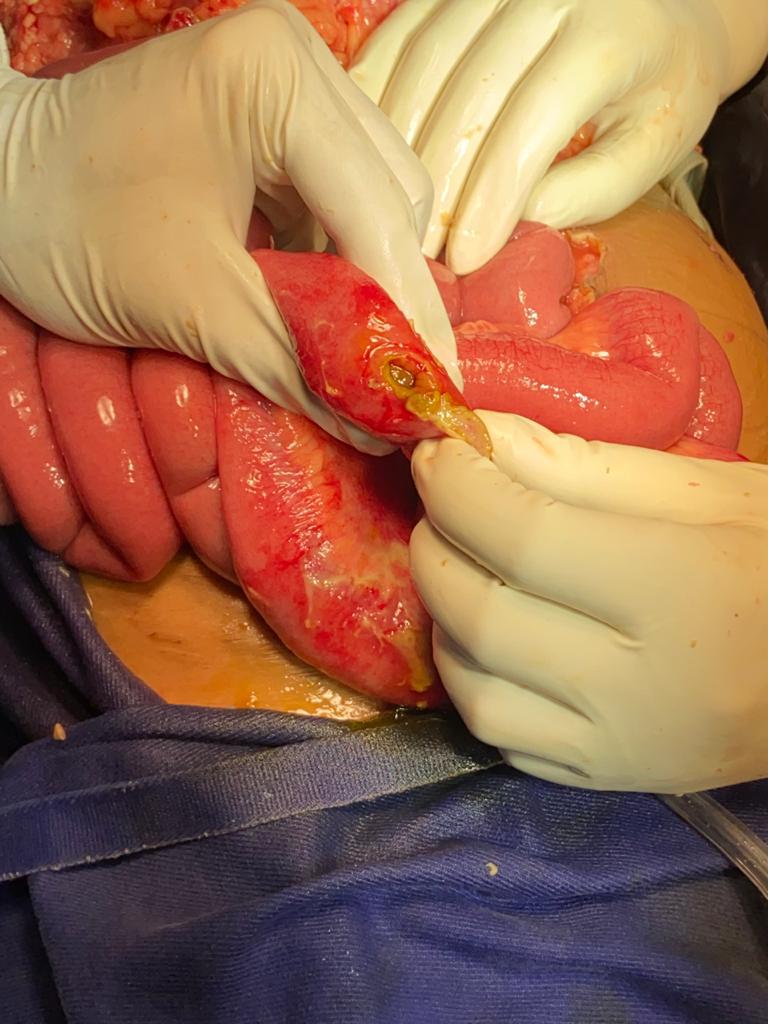
5.7.21 The abdomen was opened through midline incision for a full laparotomy and it was found there was a big mass of adherent small gut loops which could not be separated; hence the mass was excised and an end-to-end anastomosis (ileo-ileal) was performed.

This time she recovered very fast and very satisfactorily, passing stool and flatus on 2nd postoperative day, and started with oral intake 4th day onwards. Ready to be discharged home today (14.7.21).
Cervical polyp
Posted on: June 13, 2021
13.6.21
A big cervical polyp was removed along with the TAH and BLSOP (Dr Shalley’s case).

28.3.21
An obese man, Tejinder Singh (c/o Balwinder OTA) thought to have inguinal hernia gave great difficulties at inguinal exploration, the fluid of hydrocele present in the cord itself gave the appearance of a big direct or possibly sliding inguinal hernia and the cord dissection took a very long time. Eventually a small indirect sac was found but some more cord dissection led to a lot of fluid appearing in the field. It was all sucked out and the mesh repair performed. More than two months later the patient presented with a large hydrocele refilling and venereal warts on his prepuce and glans. So, after treatment of his genital warts, hydrocelectomy with epididymoorchiectomy had to be done on 23.6.21.
2.4.21
A monopolar diathermy small bowel injury during laparoscopic tubectomy (by gynae) about 5 days back resulted in peritonitis and gas under the diaphragm on x-rays. At urgent laparotomy by the assistant professor (Dr Abhishek), a thorough wash of the peritoneal cavity was done and the perforation exteriorized.
3.6.21
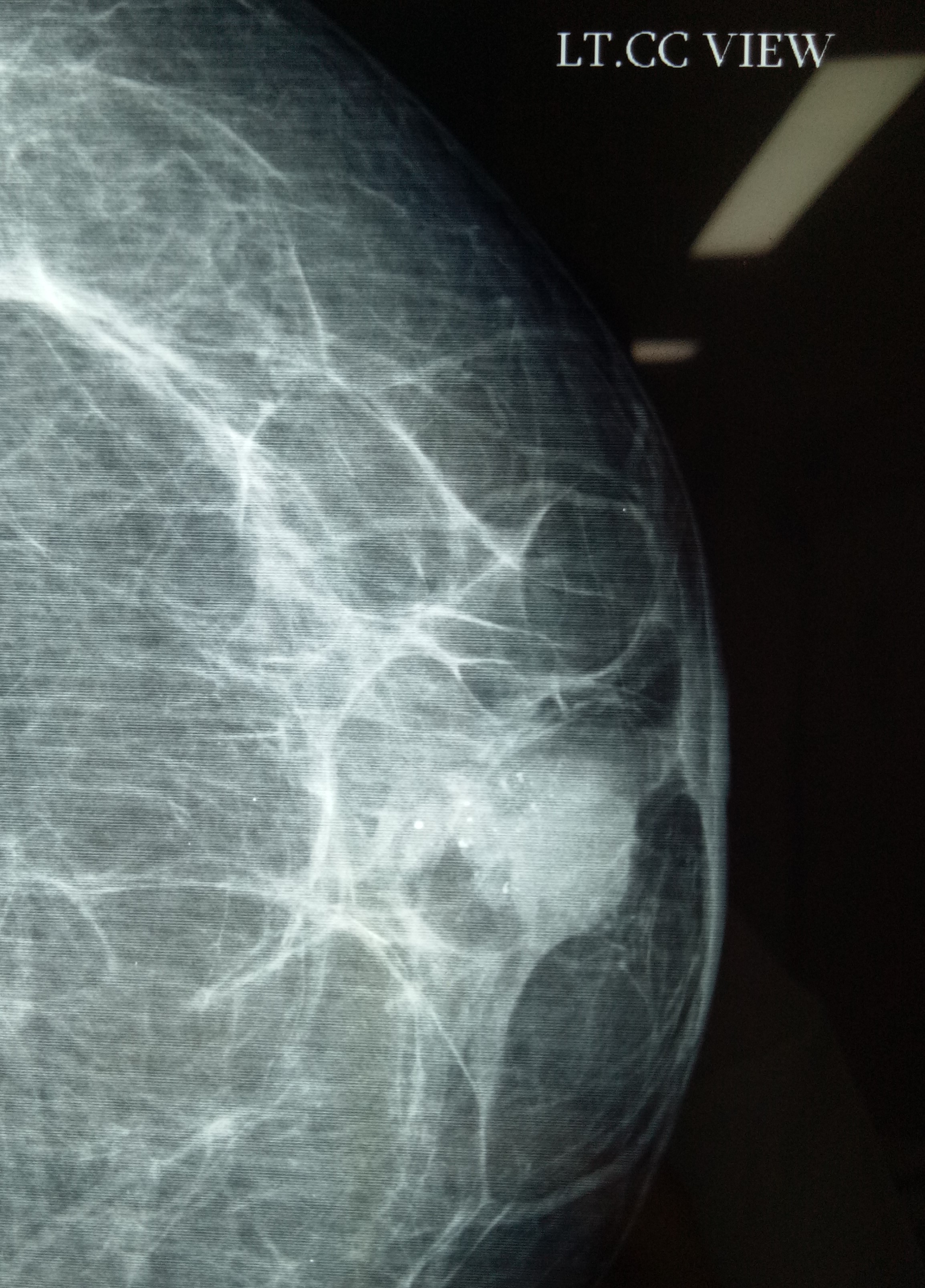
MRM for lobular carcinoma of breast (Dr Jagga’s case). Small tumor (less than 4 cm) and not expected to have metastases in axillary lymph nodes (which were not palpable) actually turned out to have a mass of several enlarged lymph nodes during axillary exploration.

18.10.20
An interesting encounter with gall stone disease: A 55 years old female (mother of Neetu, worker in OT of Shalley hospital), obese and diabetic and hypertensive was known to be carrying gall stones for many years. She landed up in septic shock (cholangitis) and severe pancreatitis and jaundice. Was luckily resuscitated and survived. An urgent ERCP (dr Atul) and stone extraction and stenting the bile duct followed. She reported passing her stent per rectum about 3 weeks later. Luckily the subsequent lap chole was not very difficult.
28.11.20
Another lesson in lap chole: an apparently easy lap chole (as per dr Jagga’s opinion) in a 55 years old female turned out to one of the most difficult and took more than 3 hours. First of all, the duodenum was adherent high up to the fundus which was very thick walled. This was carefully dissected safely. Next the cystic duct was thick walled and friable and the vicryl ligature cut through. Luckily the stump then could be clipped with two large clips. Thirdly, when beginning the dissection of the gall bladder it appeared as if the infundibulum was actually below where the cystic duct had been clipped. But by careful further dissection a safe plane behind the gall bladder could be created and what looked like the infundibulum was actually an large cystic lymph node (fallacy of perception).
Open CBDE
Posted on: June 13, 2021
27.7.20
Open cholecystectomy and CBD exploration after 4 failed attempts to clear the duct endoscopically, including two in the PGI.
5.9.20
An unusual encounter with a a femoral hernia in 60 years old male (s/o old retired laundry incharge RHP) who had been diagnosed as irreducible inguinal hernia. It actually turned out be not inguinal but femoral and mesh repair could be done through the inguinal incision itself.
7.10.20
A lap chole in a 45 years old male had to be converted due the the thick and big omental cake inseparably adherent to the thick walled gall bladder and duodenum. Even at open surgery, the procedure turned out to be very difficult due to dense adhesions around the Calot’s triangle.
16.10.20
Huge bilateral sliding inguinal hernias in an elderly gentleman (related to dr KD Singh, ex-principal GMC Patiala) who was carrying these hernias for more than 10 years. Took more than 2 hours for the bilateral mesh repair.
Locating an undescended testis laparoscopically, and a fallacy of perception in lap chole
Posted on: June 13, 2021
11.6.20
Called by dr Vikram while operating for right undescended testis in a 25 years old male but unable to find the testis in the inguinal canal.
The testis was easily located in the abdomen laparoscopically and removed laparoscopically through the inguinal incision already made.
22.7.20
An apparently easy lap chole became difficult due to two unforeseen problems – firstly due to the gall bladder being intrahepatic and secondly due to the small stones stuck in the fibrosed neck above which the gall bladder apparently narrowed down to the calibre of the cystic duct.
The first problem (the intrahepatic gall bladder) led to difficult and bloody dissection of the cystic artery which was eventually controlled. The second problem caused a fallacy of perception giving the appearance of the cystic duct to the infundibulum of the gall bladder. The dissection here too became very difficult and led to a tear in what was taken to be the cystic duct. A reappraisal of the thought process led to some dissection very low down and deep down to eventually find the real cystic duct just below the fibrosed neck of gall bladder with small impacted stones in it.
Just another example of visual fallacy of perception that so often causes trouble in lap chole.
Ileo-ileal intussusception
Posted on: May 15, 2020
15.5.20
A 50 years old male with a history of recurrent abdominal pain was diagnosed with gallstones and multiple lipomas in the terminal ileum on CT scan. After lap chole by Dr Vikram, a lower limited laparotomy was performed to discover an ileoileal intussusception and the segment of terminal ileum was excised. Cut specimen showed multiple benign looking masses.



