Archive for the ‘Uncategorized’ Category
Two bad experiences – messed up piles, fissure (Munchausen syndrome) and appendix cases. Examples of poor preoperative planning and preparation
Posted on: June 13, 2023
25.1.23
A 45 years old female had been posted for surgery for piles and a possible fissure too. At operation, the patient turned out to be very uncooperative, moving restlessly and talking incessantly and loudly. The anaesthetist had to use propofol to the spinal anesthesia to calm her down. An examination under anesthesia revealed no piles and no fissure, albeit a small perianal posterior skin tag was present. This was just excised. The anesthetist during the procedure had revealed her history of 4 previous surgeries for similar complaints. Munchausen syndrome was suggested as the possible diagnosis and was agreed to in the end with the treating physician.
The other case, a 45 years old male, was posted for appendicectomy. At operation, on palpation under anesthesia, a firm fixed mass was palpable. Again during surgery, the anesthetist gave the history! The patient had had pain for 4 months, was an opium addict and continued to neglect his symptoms. The incision had to be extended (RM), and a retrocecal chronic abscess and appendix were found with great difficulty. The pus was drained and the cavity washed clean after removing the appendix.
A 50 years old female was reportedly operated for cholecystectomy – an open operation, which was reportedly abandoned due to adhesions, as per the relatives’ version as there was no medical record available. However, a trial of laparoscopic approach was found to be quite easy and unremarkable. Possibly the operator was a beginner.
11.1.23
Another 50 years old lady had been having repeated scans (US and MRCP) reporting a contracted gallbladder with stones. The MRCP report also mentioned an ‘indentation’ on the main bile duct, suggesting pressure by a stone. At lap chole, the gallbladder was actually of normal size, albeit packed tightly with stones. The Calot’s dissection was difficult due to these stones, and the short cystic duct, dissected with difficulty, was ligated with no 1 vicryl.
27.12.22
A 50 years old male patient had to suffer for more than a year with different manifestations of gallstone disease:
Admitted with a local practitioner with acute pain RUQ abdomen, diagnosed as acute cholecystitis due to gallstones, largest stone being 14.5 mm. The ultrasound also reported wall thickening of the gallbladder wall, suggesting a longer history of the disease.

On 30.11.22, he was admitted again with a more severe attack of similar pain. This time, the ultrasound showed diffusedly thickened walls of the gallbladder, multiple stones and a possible collection in the fundal region, suggesting a perforation. A CT scan was suggested.

This reported distended gallbladder with diffusely thickened walls and multiple stones.
On 27.12.22 was admitted for lap chole. An US this time showed a wall echo complex in the gallbladder fossa. A routine lap chole was performed, resulting in the end of the suffering.
Neglected phimosis can lead to diagnostic confusion – posterior urethral valves vs neurogenic bladder?
Posted on: June 5, 2023
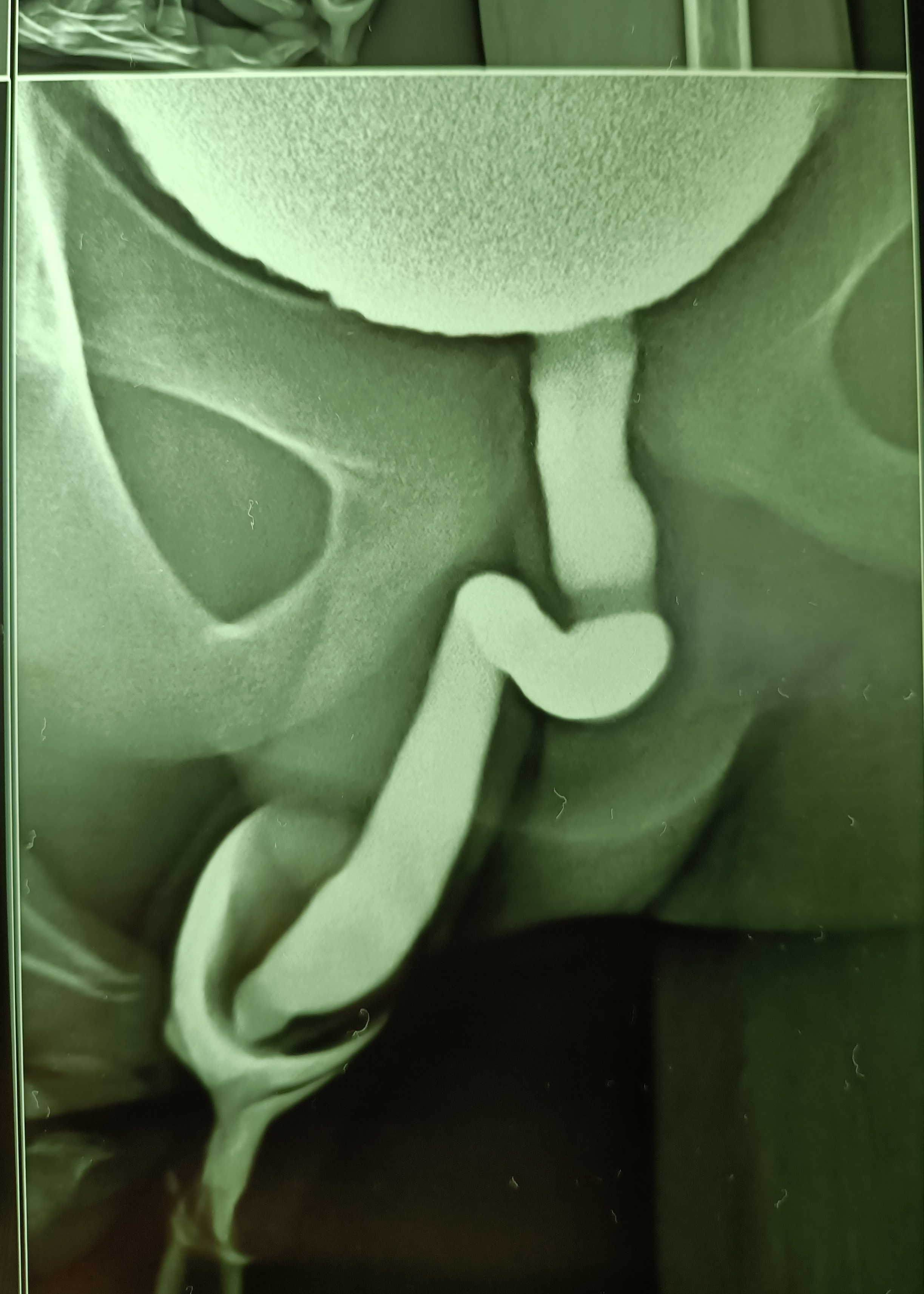
A 13 years old boy presented with acute painful retention of urine at night (it was actually an acute-on-chronic retention, as it came to light later) and since catheterization could not be done due to the tightly stenosed preputial opening, the bladder was emptied with a suprapubic needle. An ultrasound scan in the morning reported circumferential wall thickening of the urinary bladder and a V-shaped deformity of the bladder neck, suggesting a diagnosis of posterior urethral valves.


Paediatric surgical consultation was obtained and an MCU was suggested. This was done and suggested a diagnosis of neurogenic bladder while ruling out posterior urethral valves.

A routine circumcision was performed the same day and the child remains well thereafter.
Two lap chole lessons in one day
Posted on: June 4, 2023
19.10.22
lesson 1. Gallbladder tightly packed with small stones is better emptied of all its stone burden to make dissection easier and safer:
A 55 years old lady was admitted for lap chole after a 3 days hospitalization in some other hospital for acute pancreatitis from which she had recovered. The fact that the gallbladder was tightly packed with stones was not apparent by the look of the gallbladder, but the dissection of the cystic duct and its clipping took a long time due to small stones in it which had to be milked up repeatedly. During dissection of the gallbladder from its liver bed, its wall ruptured spilling hundreds of stones, and when all stones were removed, it was realized if we could have done that intentionally before dissection of the cystic pedicle, it would have made the procedure more safe and easy, and perhaps taking lesser time than it took otherwise.
lesson 2. A Kocher clamp with stout teeth can be very helpful in breaking big hard stones:
A lap chole in a 60 years old lady was rather easy as far as the dissection was concerned, but the single big stone (2.7 cm) caused problems in taking out the gallbladder through the epigastric port. It could not be broken into pieces with the usual ovum forceps or the bigger clawed instruments, but then the scrub nurse suggested to use the long Kocher clamp’s sharp teeth, which were eventually able to break the stone into pieces, so as to remove it without enlarging the port.
A young girl, 17 years old, sustained multiple left lower rib fractures and a splenic injury. Was stable hemodynamically, and was managed conservatively. However, CT scan showed a grade IV injury, with a 1.5 cm pseudoaneurysm, for which she was referred to PGI for embolization.
2.9.22
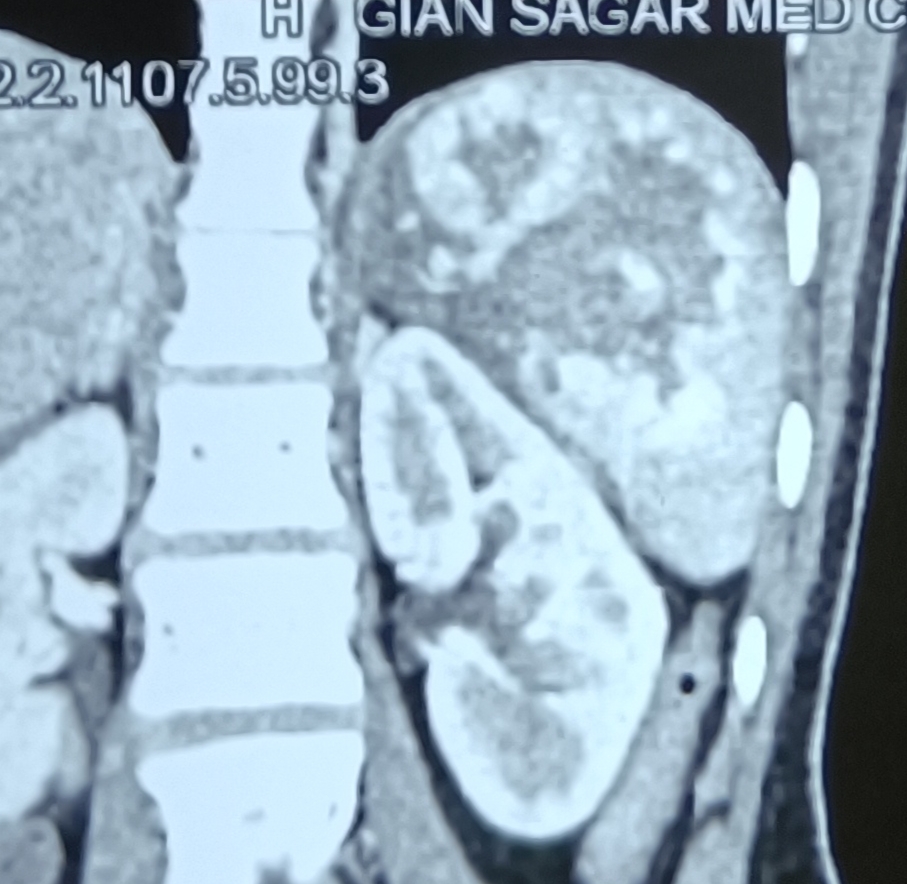
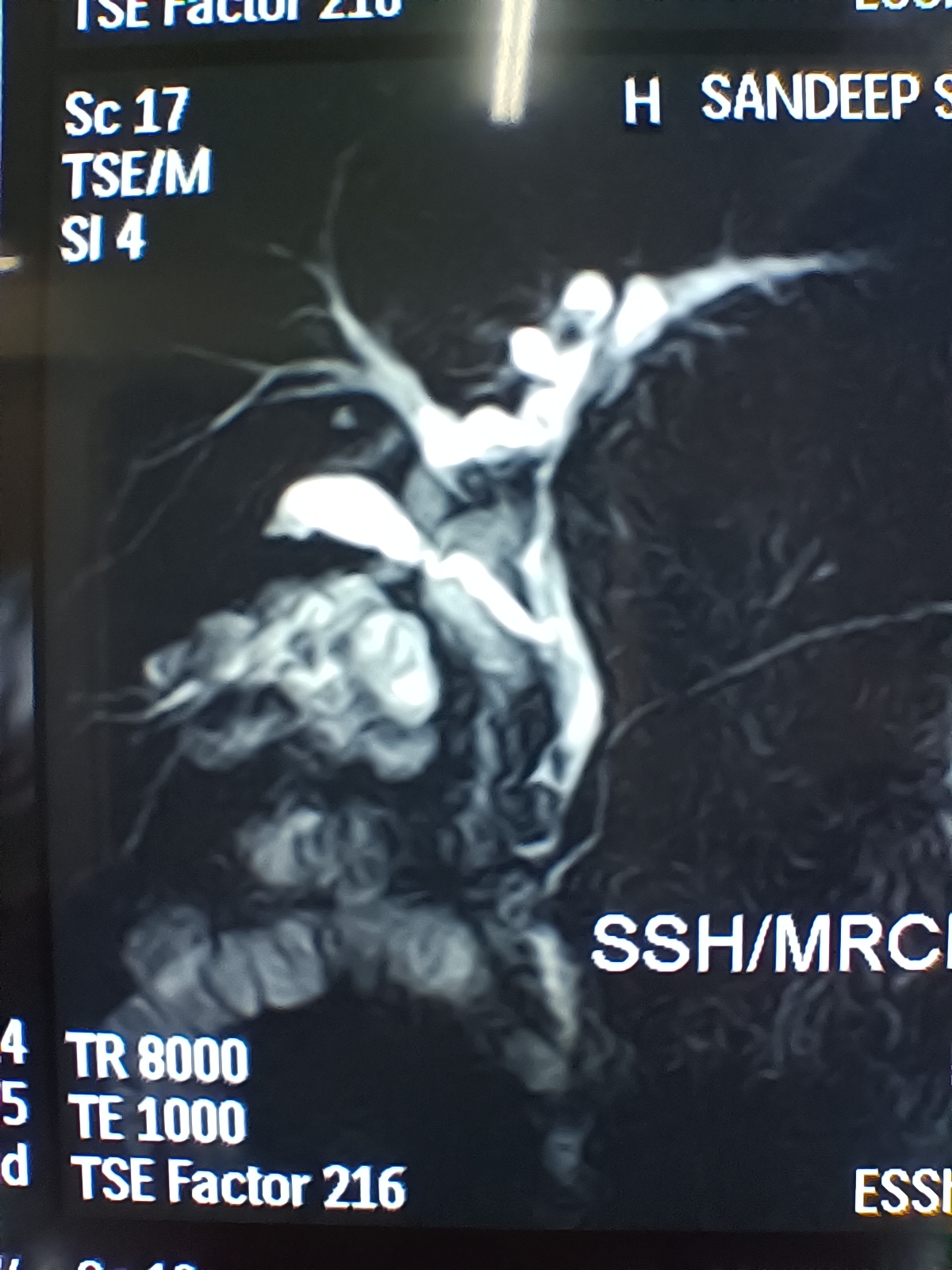
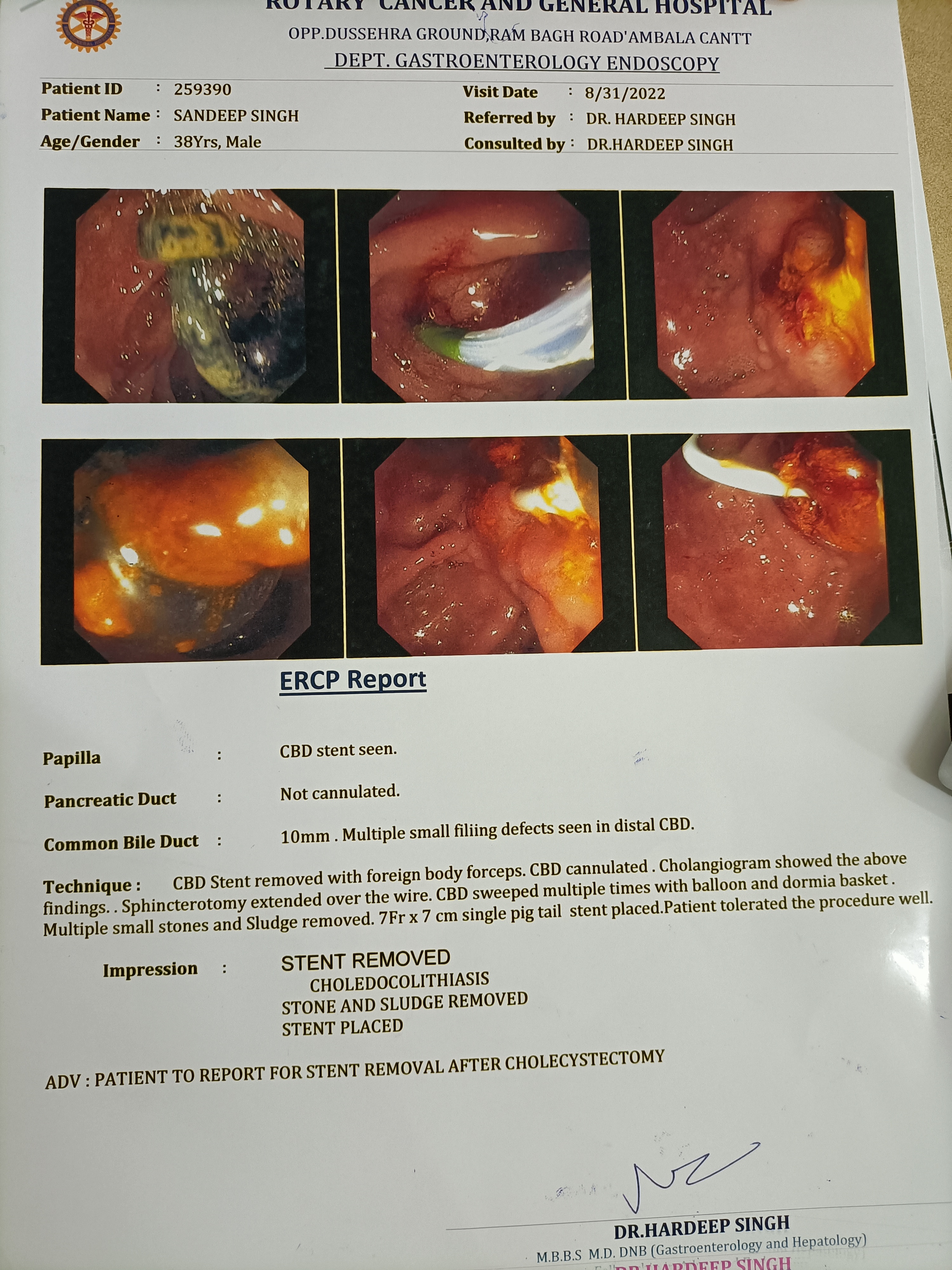
Sandeep singh, 40 years old male patient. Had ERCP, bile duct clearance of stones and stent placed in the bile duct by Dr Arya at Patiala about one and a half years back. Didn’t have cholecystectomy. Presented now with cholangitis. ERCP again, stone and sludge removal from the bile duct and placement of a new stent was done. Lap chole was easy. The ultrasound showed contracted gallbladder, while the MRCP showed a well distended gallbladder and a long cystic duct.
19.9.22
Amrik Singh 78 years old male (c/o dr Mohi). Big distended gall bladder, the fundus was palpable well below the costal margin (ram-horn gall bladder?). MRCP showed a long cystic duct, but at surgery, dense omental adhesions were found and removed with the help of harmonic scalpel, and the gallbladder was emptied first of its load of multiple big stones. The cystic duct could still not be clearly defined. Therefore, the gallbladder was ligated at its neck, and removed piecemeal.
20.9.22
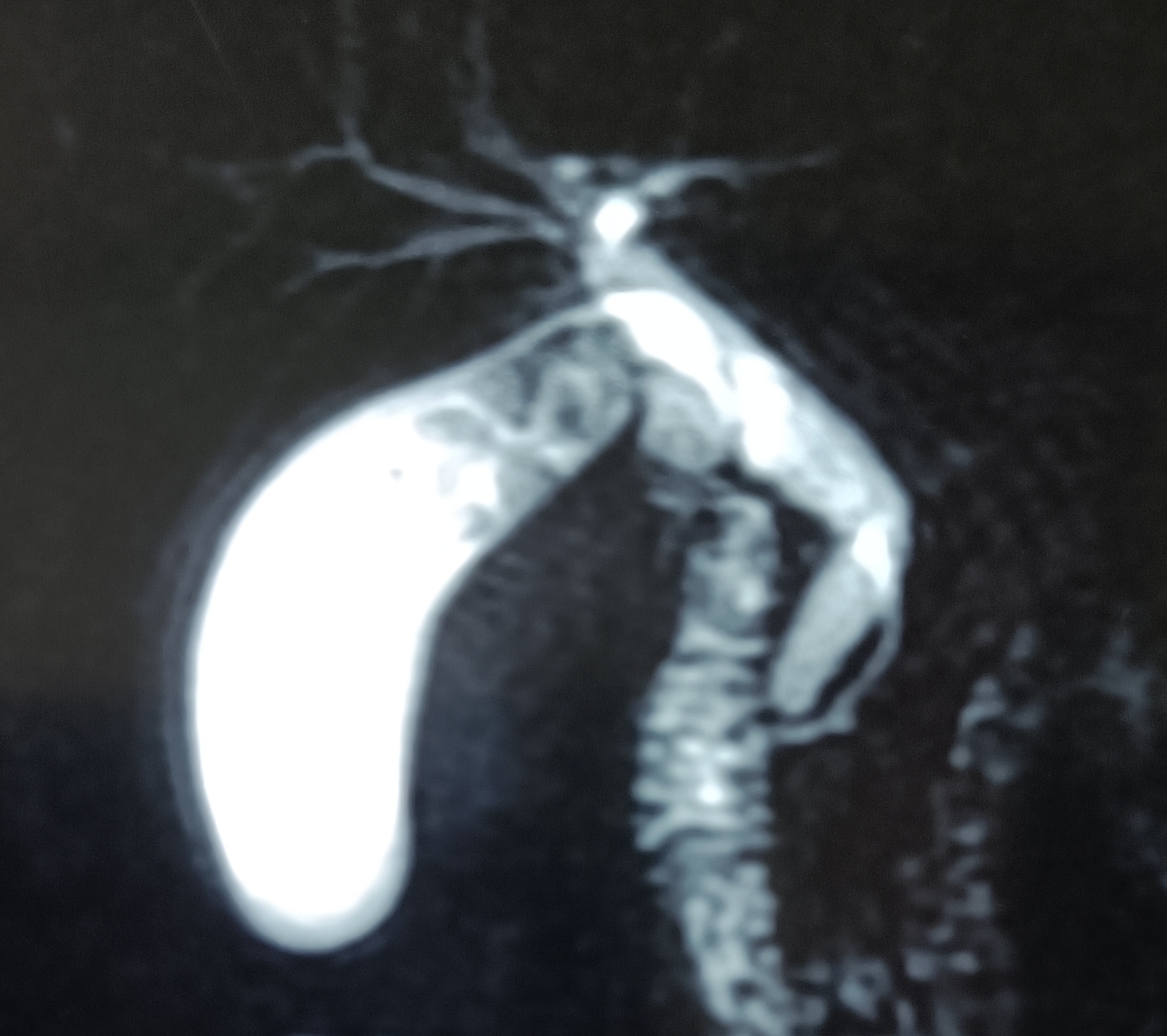
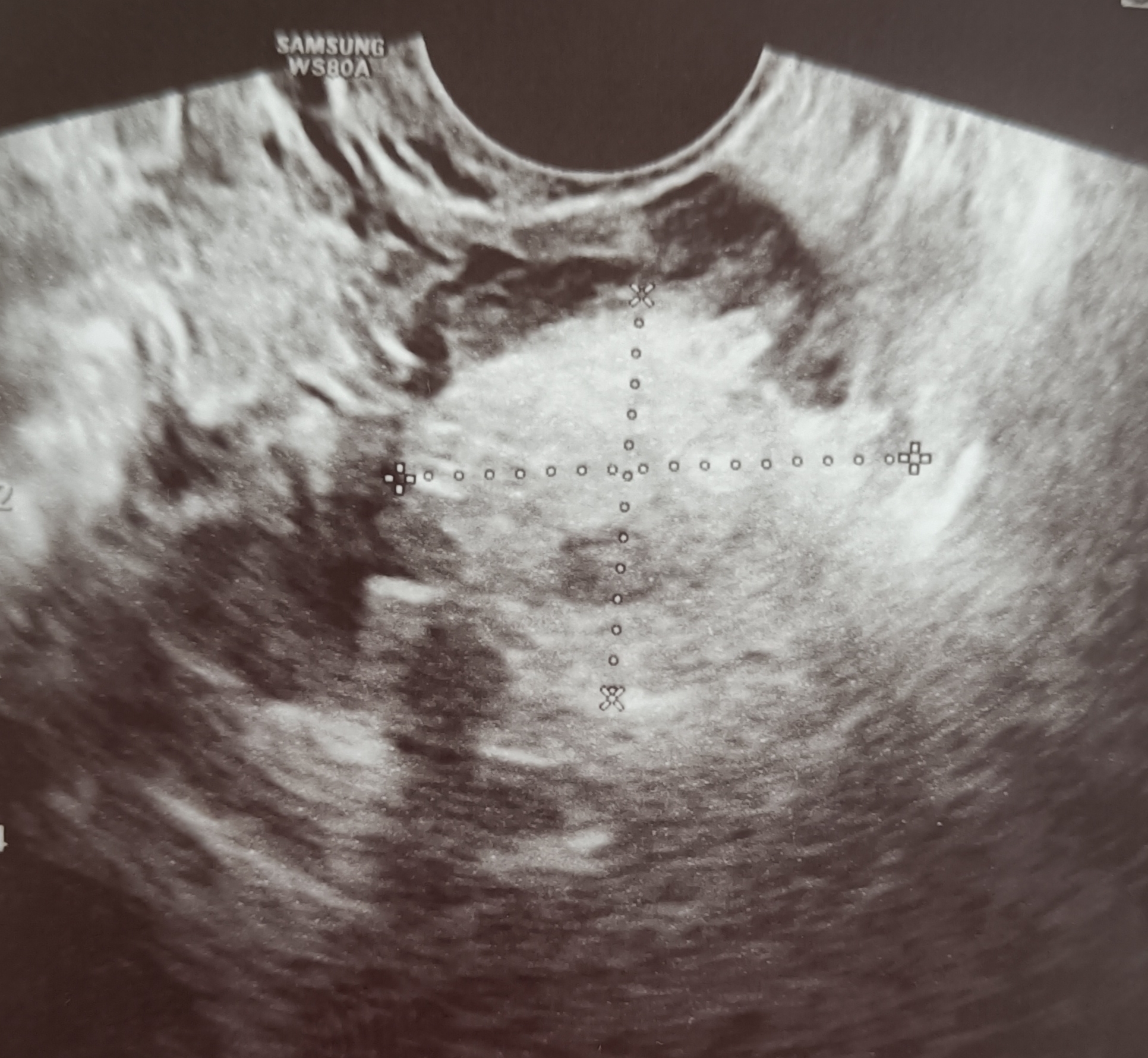
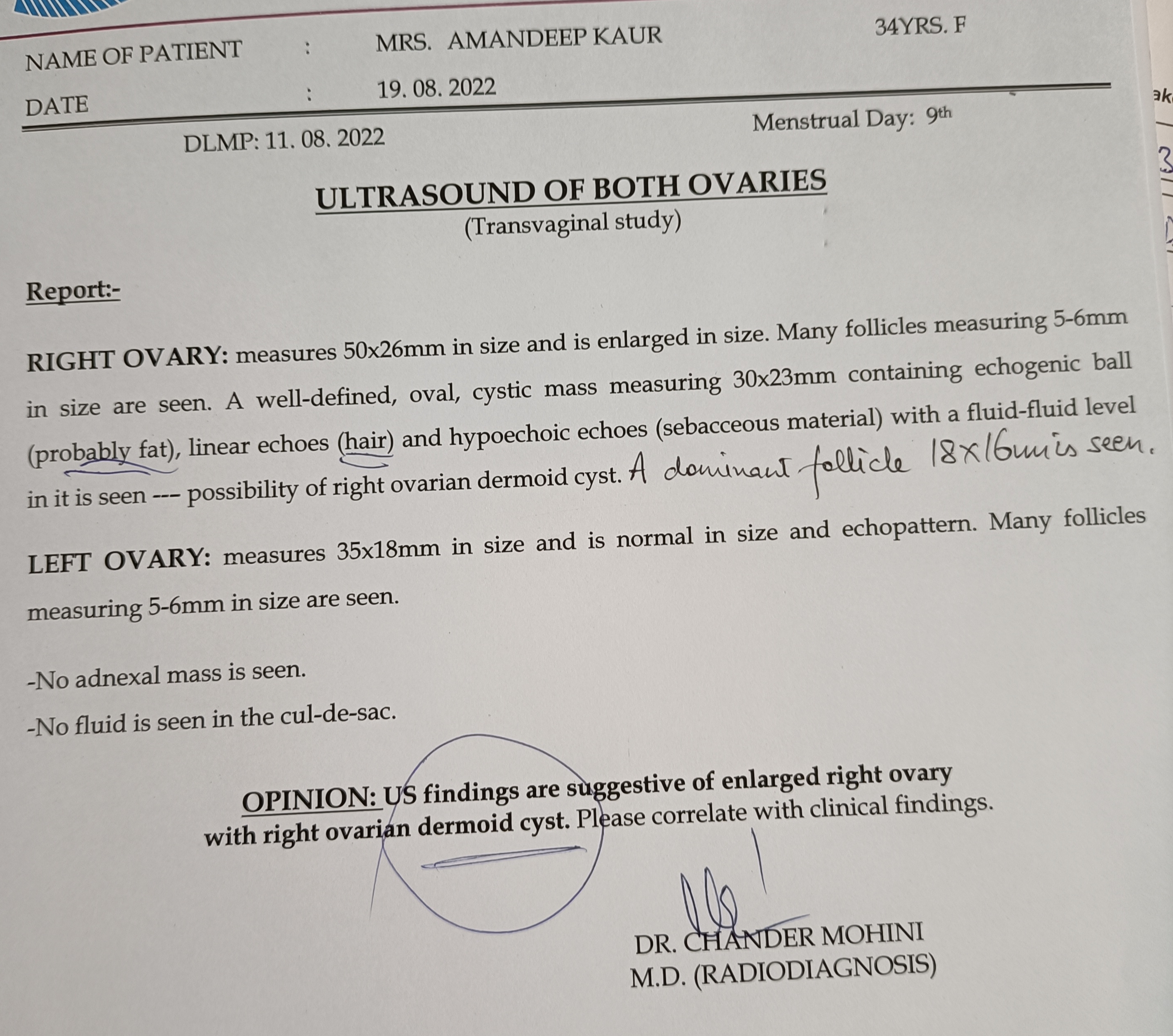
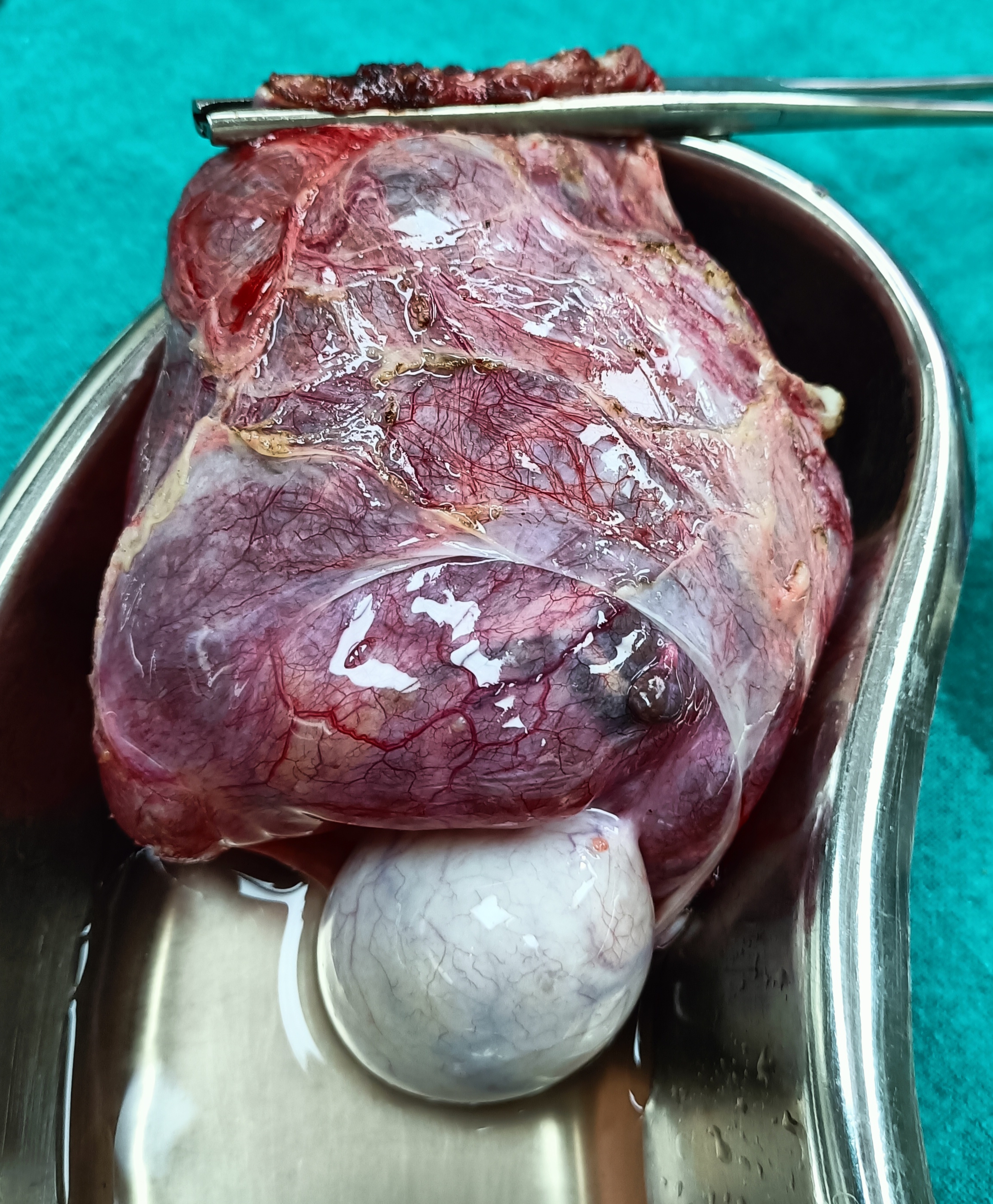
Amandeep Kaur, 35 years old female. Had a previous history of left salpingectomy done for ectopic tubal pregnancy in the left tube. Ultrasound now showed a dermoid cyst in the right ovary. The cyst was removed laparoscopically while preserving the ovary. The cyst showed a tuft of hair, and the biopsy report showed some skin elements too (ectodermal element).
Big epididymal cyst/tumor. A hospital employee (in GSMCH), 35 years old, presented with a big scrotal swelling, diagnosed as hydrocele on ultrasound scan. At operation, there was scant amount of fluid around the testis, and instead, there was a big epididymal swelling, rather inseparable from the testis. Therefore, an epididymoorchidectomy was performed. Biopsy report later turned out to be an epididymal cyst, not hydrocele.
Appendicoliths causing appendicitis in a 4 years old child, and a cancer of the lips caused by zarda addiction
Posted on: August 10, 2022
3.8.22
A 4 years old male child with clinical features of appendicitis was found to have a big pelvic appendix with two big fecoliths in the lumen; the bigger one near the tip and causing a palpable mass adherent with the right superolateral wall of the urinary bladder. The incision had to be extended medially to locate the appendix and carefully separate the mass at its tip from the bladder.


15.7.22
A poor man (rehriwallah), 50 years old, had a non-healing ulcer on the left angle of the mouth. He had been a zarda addict for decades. Biopsy revealed a squamous cell carcinoma.

Difficulties encountered:
big gall bladders and big Hartmann pouches in those done on 8,9,10,24 june, and on 2, 4, 7 july:
Most had to be aspirated to make them smaller, some opened up to empty them of all stones. The big Hartmann pouches had to be carefully lifted up and dissected slowly.
The one done on 8.6.22 had a band like vessel causing pressure on the H pouch. On division of the band with vessel (cystic artery) in it, the pouch became one with the gallbladder. Thereafter, the cystic duct was found to be non-existent, and gallbladder was deemed to be sessile; hence endo-ligated at the neck and divided and removed.

3.7.22
A most difficult lap chole; entirely unexpected from reports. A 50 years old male police inspector. Lap chole had to be converted to open after finding that the adhesions with duodenum were inseparable and that further efforts might end up in a duodenal leak. At open operation, blunt finger dissection opened up an empyema which was cleaned up. The big stone in the neck of gallbladder was removed. Rather than attempting to separate the gallbladder from the duodenum, some wall of the gallbladder was left with the duodenum and the remaining walls of the gallbladder were removed, thus leaving behind the frozen Calot’s triangle as such. The fossa from where the stone was removed revealed a small bile leak, presumably from the pressure of the big stone causing some erosion of the bile duct, and a drain was kept. It drained small amounts of bile till 27th of July and then dried up.
Patent processus vaginalis (PPV) dissected out at herniotomy for congenital hydrocele, and two very contrasting lap choles
Posted on: May 29, 2022
25.5.22
The patent processus vaginalis causing hydrocele in a 5 years old child was neatly dissected, ligated at the internal ring and then excised after draining the hydrocele fluid. Photos taken by second year medical students.

19.5.22
A 62 years old male was admitted with history of severe pain and jaundice, caused by gall stones and CBD stones. At ERCP, a single stone was removed from the common bile duct after a sphincterotomy. Lap chole the next day turned out to be very difficult, bloody and prolonged. The small gall bladder was removed in pieces after ligating the wide cystic duct with vicryl.
21.5.22
A 35 years old female had the gallbladder reported as shrunken at US, and an MRCP showed a distinct but small gall bladder. The lap chole turned out be very easy.
