Archive for the ‘operations’ Category
Hepaticojejunostomy for BDI, wrongly diagnosed cystic pancreatic tumor, twisted ovarian cyst, GB empeyma, TEP repair, ABSI conference and a free medical camp
Posted on: June 9, 2013
25.4.13
BDI (at lap chole 18.3.13) repaired by Roux-en-Y hepaticojejunostomy. High (type III) injury at hilum, both ducts (right and left hepatic) exposed at hilum, left duct exposed further by lowering the hilar plate and enlarging its lumen to avoid stricture later. Follow up so far satisfactory.
6.5.13
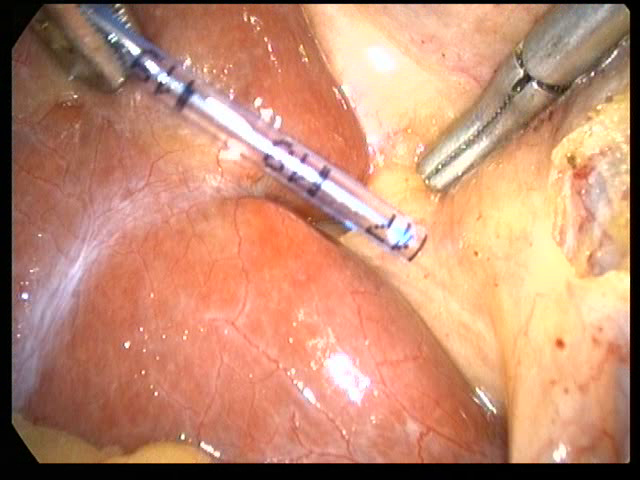
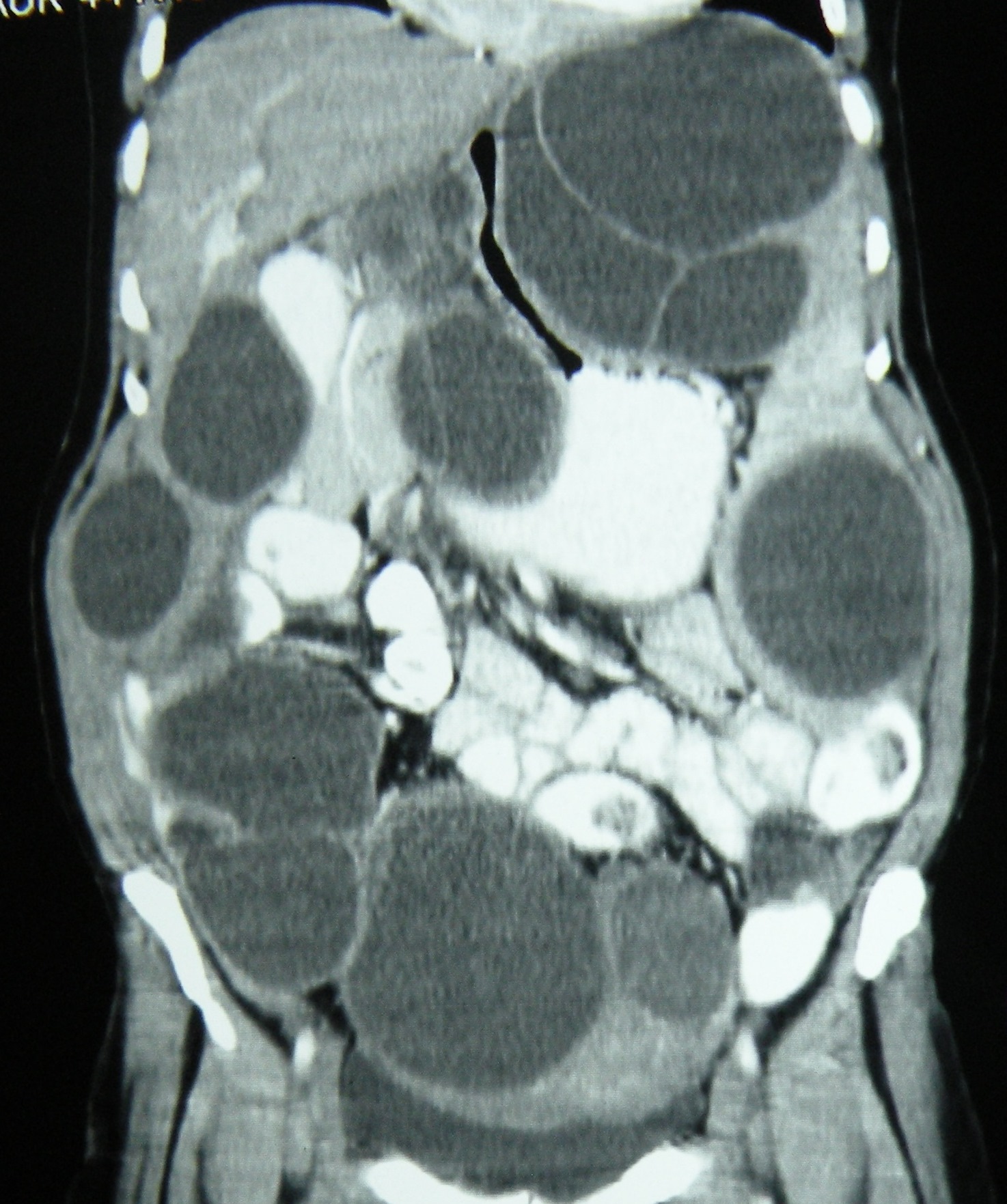
A 25 years old female, with a CT diagnosis of hepatic hydatid taken up for laparotomy. Turned out to have a retroperitoneal cyst on exploration, and on further dissection was found to be arising from the head of pancreas (?cystic neoplasm of pancreas). A large amount of haemorrhagic fluid aspirated and a lot of degenerated material evacuated from within the cavity, the walls of which were also excised. May need resection of pancreas later, depending on the biopsy report.
9.5.13
A difficult lap chole in a young Nigerian (undertrial here for drug trafficking) male, with a thick walled empyema, neck of gallbladder ligated, and the gallbladder removed piecemeal.
13.5.13
Lap chole in a young (20 y o) male with spherocytosis. Will have splenectomy later.
16.5.13
A young unmarried girl from gynae (dr khushpreet’s case) with bilateral ovarian cysts, for laparoscopic removal. Large left cyst had twisted, the thick walls removed piecemeal, the right one was a small paratubal cyst, removed intact.
17.3.13
Attended the annual ABSI conference at PGI Chandigarh. Lectures mainly on breast reconstruction.
30.5.13
TEP repair of right inguinal hernia in a tall young (25) rural man, addicted to bhukki and alcohol. Complete sac, transected and reduced.
2.6.13
A free medical camp organized by Akal academy, held at Cheema sahib in Mansa district. Examined more than 50 patients with surgical problems. Will be taken up for free surgery.
6.6.13
Displaced Cu-T found, at laparotomy, to lie embedded in the omentum part of which was excised. An earlier attempt to find the Cu-T at laparoscopy had failed on 22.2.13.
Lap chole 45 F, easy. Small Rouviere’s sulcus.
Failed attempt to find displaced copper-T, lap excision of renal cyst, a Dutch lady’s lap chole, appendix abscess in a 60 years old woman,a partial bile duct injury and intraperitoneal hydatids.
Posted on: April 4, 2013
- In: operations
- 1 Comment
22.2.13
A laparoscopic attempt to find a displaced copper-T failed. Later found at open surgery to be concealed in the omentum, which had completely wrapped itself around the copper-T.
4.3.13
A wrongly diagnosed ovarian cyst (young unmarried woman 22 years old) went for a laparoscopic removal, but at operation, it was found to be too big and more solid than cystic, so converted to open removal. Path report – Leydig Sertoli tumour.
7.3.13
Bilateral TEP repair of inguinal hernia in 45 years old man, smooth and simple.
Laparoscopic excision of symtomatic renal cyst in a 62 years old man was easy.
Lap chole in a 50 years old Ducth lady was difficult. The gallbladder was packed with big stones, all had to be removed first, then chole was easy.
14.3.13
Laparotomy in 60 years old woman with appendix abscess and an autoamputated appendix. Pus drained, and appendix removed.
18.3.13
Most difficult lap chole. 50 years old female, dense omental adhesions took more than half an hour, dense adhesions with duodenum took more than one hour, then a big stone in neck had to be removed to gain access to calots triangle, stones removed but cystic duct was misidentified for dense adhesions in middle of gallbladder fossa and cauterised to leave a hole in it, which drained bile postoperatively for a long time. ERCP failed to identify CBD and stent it. The bile duct injury was repaired by Roux-en-Y hepaticojejunostomy (left duct approach) on 25.4.13. The upper CBD had disappeared (cautery damage?), leaving the two hepatic ducts open at the hilum. Postoperative recovery was entirely satisfactory, so was the follow-up.
4.4.13
Intraperitoneal and retroperitoneal hydatids in a 55 years old woman, all excised over a period of more than 2 and 1/2 hours.

13.12.12
TEP repair of inguinal hernia on a 60 years old man, the inferior epigastric pedicle got detached but no further problems with dissection.
18.12.12
Held a clinical meeting in ME cell of the college, wherein two rare presentations of tuberculosis of the vertebral spine were discussed. The cases were presented by Dr BL Bhardwaj, professor of medicine.
15.1.13
A very difficult empyema of gallbladder in a 60 years old man. Lap chole by opening the gallbladder first, emptying it of stones, and then fundus first dissection, and then ligating at the neck.
19.1.13
Herniotomy in a one year old female child with right inguinal hernia. The contents were the ovary and fallopian tube, saw this for the first time.
21.1.13
Trichobezoar removed from the stomach of a 5 years old female child.


A difficult incisional hernia, a TEP repair, a chronic breast abscess and 2 difficult gallbladder empyemas
Posted on: July 19, 2012
16.7.12
An incisional hernia following cesarean section 20 years back in UP. Uterus and bladder adherent to abdominal wall through the hernia. UB got injured and was repaired. A large mesh to repair the defect. Satisfactory recovery.
19.7.12
A bilateral TEP repair in a 65 years old man. Left hernia bigger and direct; the right one indirect and smaller. Bilateral mesh implant.
19.7.12
A young female (30 yrs old) with a breast lump – reported to be tubercular in nature on FNAC. At excision under GA – turned out to be a thickwalled abscess with thick pus inside. The whole wall of the abscess excised and sent for biopsy.


Two difficult empyemas of gallbladder. The first one, preoperatively thought to be easy on US and LFTs, a younger 30 years old female, surprisingly turned out to be tense and turgid, full of pus which was aspirated. The duodenum was densely adherent, but was dissected away. The big stone in the neck came in the way of dissections and so was taken out first. The the cystic duct could be identified but the cystic artery could not and was simply coagulated. The gall bladder had to be cut into 6 pieces to remove because it would not come out thru the 1 cm port.
The second one was not as difficult but turned out to be sessile gallbladder with a previous history of ERCP and ES for duct stones. The gallbladder was simply ligated at the neck with no 1 vicryl.
Misidentification of anatomy at lap chole, and giant condylomata acuminata
Posted on: February 15, 2011
- In: operations
- 2 Comments
13.11.2010
Misidentification of anatomy at lap chole caused panic. The lymphatics and fat with the cystic lymph node on top were identified as cystic artery and clipped and divided as such. Next the cystic artery was misidentified as cystic duct and divided as such after clipping. When the real cystic duct came into view, there was panic all around in view of the consideration that the main bile duct may already have been clipped and divided below having been misidentified as the cystic duct.
23.11.2010
Sternocleidomastoid tenotomy for severe torticollis in a 20 years old male.
25-28 nov. 2010
ICS conferenced attended in Pune.
30.11.2010
TEP using a light weight mesh. The sac had to be endlooped.
16-17 dec. 2010
ASI annual conference Delhi attended.
3.1.2011
Open cholecystectomy and CBD exploration after an unsuccessful attempt at endoscopic CBD clearance. Jaundiced patient. 55F. wife of Mr Jit Singh Virk. Sessile gall bladder, so the CBD stone could be milked up into gallbladder and removed without opening the CBD.
3.2.2011
Lap chole in an HIV positive 40-yr-old male, turned out to be very difficult. Dense adhesions and almost obliterated Calot’s triangle. The cystic duct could not be defined, so the gallbladder neck was endlooped and ligated.
12.2.2011
OPD pictures of giant condylomata acuminata.


Abdominal cocoon, Breast ADH turned out to be IDC, SELSICON in Patiala, lap chole for retained GB stump, and a unique trichobezoar of matchsticks. shifted to wordpress from spaces.
Posted on: October 13, 2010
30.8.10
Ginu’s counselling (2nd) at faridkot bfuhs, gets Bathinda medical college. At last!
4 and 5.9.10
SELSICON annual national conference in our college, essentially a workshop. Interesting diverse cases of endoscopic surgery shown, including urological and gynaecologic and a 6-hour laparoscopic total proctocolectomy and IPAA.
7.9.10
Breast lump (60F) excised for FNA report of ADH. Later had to do a complete MRM for infiltrating carcinoma with positive lymph nodes.
14.9.10
A recurred high intersphincteric fistula excised.
21.9.10
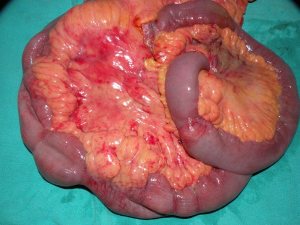
Laparotomy for an abdominal mass in 35M with a mass and intestinal obstruction. Turned out to be an abdominal cocoon. The dense fibrotic cocoon excised and intestines freed. A short segment of ileum had to be excised.
2.10.10
A bezoar of matchsticks removed from the stomach of a young male child 5 years old!

5.10.10
Lap chole for removing a retained stump of gall bladder after earlier lap chole a few months back at Barnala had left a part ( the neck ) of the gall bladder.
10.10.10
GJ for GOO 35F with a diffuse thickening of wall of distal stomach extending up to D2 which being adherent to CBD was not excised, just bypassed.
12.10.10
Two unexpectedly difficult lap choles, both young (30-35) females, both had sessile gall bladder, both had to have fundus first dissection and the neck ligated with vicryl.



- In: operations
- 2 Comments




- In: operations
- 2 Comments




{kind=link}