Archive for May 2024
4.5.24
An elderly patient (c/o Gurmukh Singh, ex-employee, gynae), 70 years of age, presented with epigastric and RUQ symptoms, with previous history of open cholecystectomy 2 years back at Malerkotla civil hospital through a small incision (so-called mini-lap).

The ultrasound scan, however, still showed a smaller rounded gallbladder.
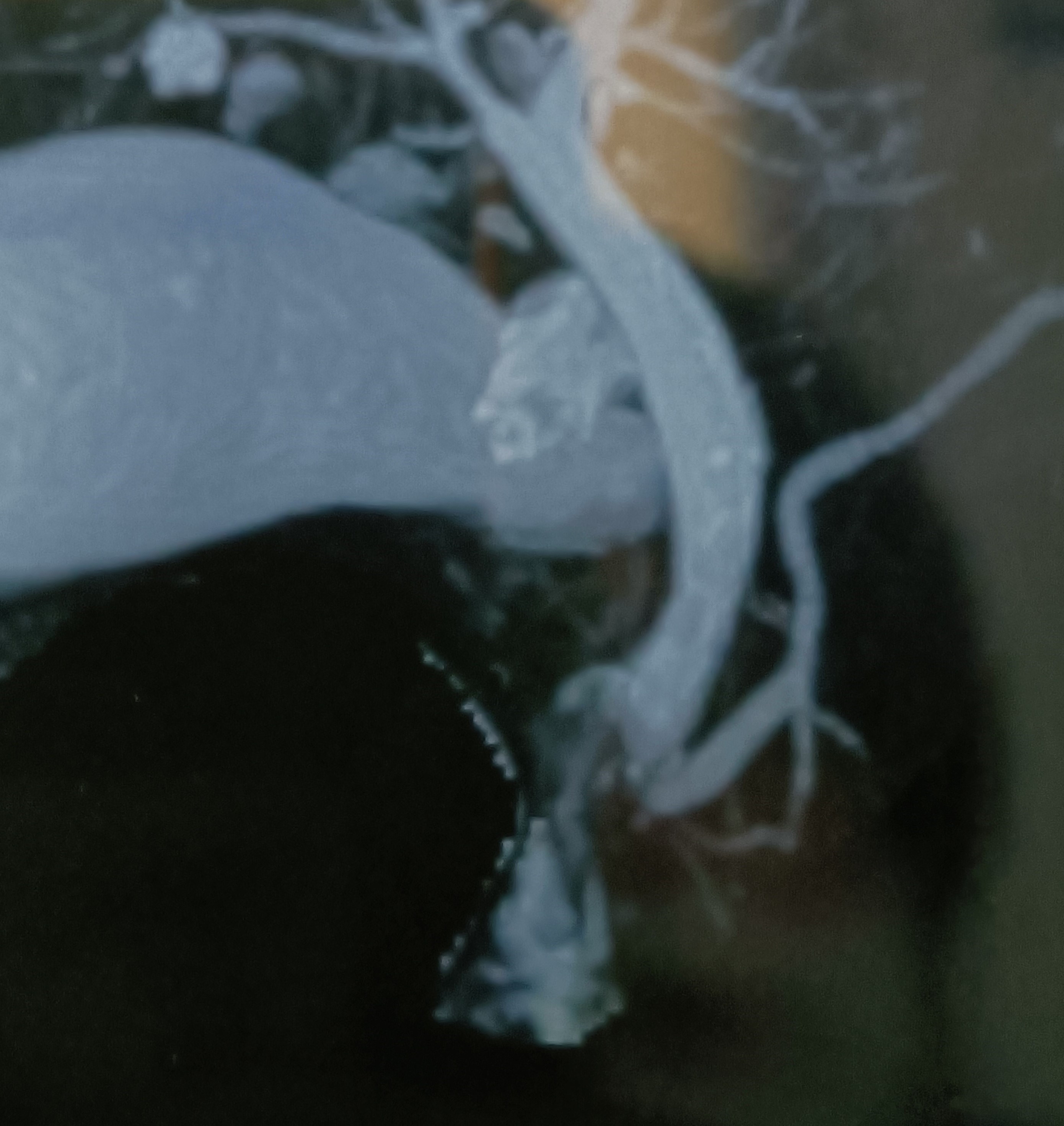
An MRCP was obtained for local biliary anatomy.

At lap chole, dense omental and colonic adhesions took time to safely dissect off the top of the gallbladder which came into view only at the middle of the gallbladder fossa.
Thereafter, the going was easy. It was a small rotund residual gallbladder, suggesting the upper half had been removed (partial cholecystectomy).
2.4.24
A 45 years old lady presented with a big painful swelling below the umbilicus which was diagnosed clinically as PUH, possibly obstructed. At operation instead, the swelling turned out to be a chronic abscess full of thick pus. Further exploration showed a foreign body emerging out of a small hole in the rectus sheath, and on enlarging the opening in the sheath, a full sized abdominal pack could be pulled out (gossypiboma), possibly retained during TAH on 9.11.23. The drain continued to drain thick pus for 3 weeks and then dried out, with full recovery.

19.4.24
Lap chole in a 50 years old female turned out to be very difficult due to dense fibrosis in the Calot’s triangle. She had a very big stone (34 mm on US) impacted in the neck of gallbladder, the stone was disimpacted and removed. Still no safe progress could be made in dissection of the area due to dense fibrosis, and the case was converted to open after 2 hours.
At open operation, the thick mass at the neck of gallbladder could be separated from the underlying bile duct which however was denuded to expose the mucosa which appeared to be intact. The drain, however, continued to drain bile for a little more than 3 weeks and then dried out.

Tuberculosis of the breast
Posted on: May 2, 2024
8.3.24
A 38-year-old lady (Dr Rajni’s patient) presented with a long-standing (more than 6 months duration as per history) inflammatory mass in the left breast – never actually resolving despite prolonged antibiotic treatment and diagnosed clinically as an antibioma. This mass (along with a sinus which had developed recently) was excised under general anesthesia. The biopsy report surprisingly came out to be tuberculosis.


Was referred to TB hospital for medical treatment of tuberculosis. There she was put on anti-tubercular drugs, starting with 4 drug combination for first two months.
Gastrojejunostomy with repair of diaphragmatic eventration, and gallstones with CBD stones
Posted on: May 1, 2024
22.12.23
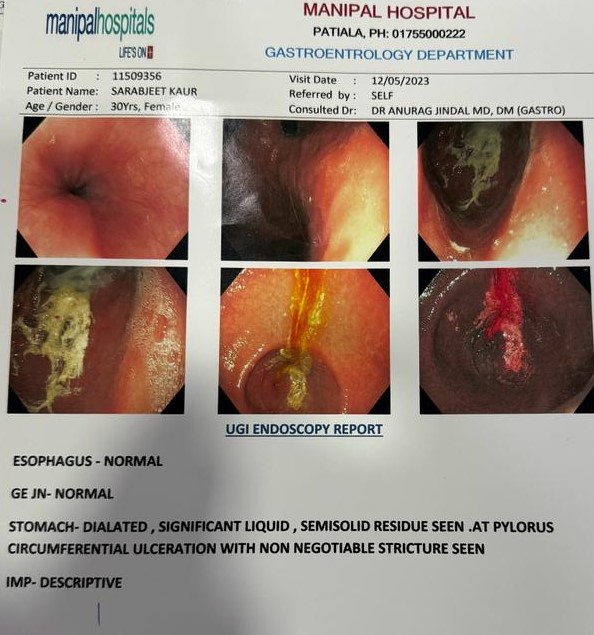
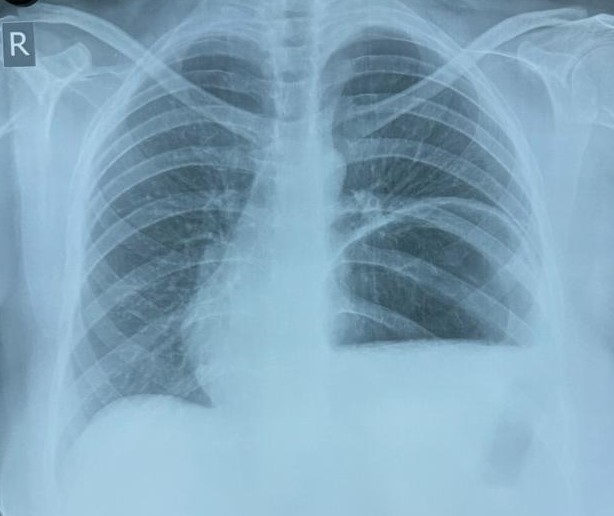
A 35-year-old female presented with features of pyloric stenosis/GOO (gastric outlet obstruction) due to chronic peptic ulcer, confirmed on endoscopy, for which a retrocolic gastrojejunostomy was performed. Also, her chest x-ray revealed eventration of diaphragm, for which the diaphragm was plicated with running layers of 1-0 prolene sutures.
25.1.24
A very difficult lap chole was done in a 60 years old male, with history of choledocholithiasis (ERCP showed a meniscus sign) too, for which ERCP clearance had already been done. The procedure took 3 hours, the Calot’s triangle was all fibrotic. Fundus first dissection up to the neck of gallbladder was done and the neck ligated below it with vicryl.