Surgical odyssey of an unfortunate patient
Posted on: July 9, 2021
24.6.21
Baljit Kaur 65 years old female

A detailed history of this patient’s journey towards several abdominal operations:
- Laparotomy (in PGI) in 1988 following enteric perforation of ileum resulting in peritonitis. The incision was long midline and vertical.
- 1992: the laparotomy was followed by an incisional hernia through that laparotomy incision; this was repaired possibly without a mesh in PGI again.
- 1996: an open cholecystectomy for gallstones was performed in Chandigarh government hospital sector 16, and they were told they also repaired through the same incision the incisional hernia which had recurred.
- 2000: An abdominal hysterectomy was performed (Shalley hospital) through the lower abdominal transverse (Pfannenstiel) incision.
- and 6. June/July 2021. The two surgeries given below starting with the incisional hernia first; and then
- a laparotomy for intestinal obstruction ending with resection of a big mass of matted small intestine which had been causing obstruction.
An incisional hernia (that had recurred perhaps for the third time) in the right upper part of the abdomen repaired in a 65 years old female. Because of the history of multiple operations earlier, a CT scan was performed and showed a defect in the anterior abdominal wall with a loop of intestine protruding.

Presuming it to be a routine case of an incisional hernia where the intestinal loop will be reduced back into the peritoneal cavity and the defect repaired, we started happily. But it turned out to be a nightmare when the loops of intestine just could not be separated from the edges of hernial defect, and it was discovered that some of these loops of small bowel were trapped in the prolene sutures used for the hernia repair earlier.
Diligently and slowly (taking nearly 3 hours, so as not to end up in a perforation) the intestinal loops were freed as much as possible through this incision and the hernia defect then defined after repositing the loops into the peritoneal cavity. The defect was then repaired with prolene sutures and a prolene mesh.
Postoperatively the patient seemed to be making good recovery for the first 3-4 days but then started having distension and vomiting, suggesting intestinal obstruction which did not respond to conservative treatment.
CT scans confirmed grossly dilated small bowel loops in the pelvis and left flank and one jejunal loop high in the centre, besides showing a mass of dense adhesions just under the staple line of the hernia surgery.

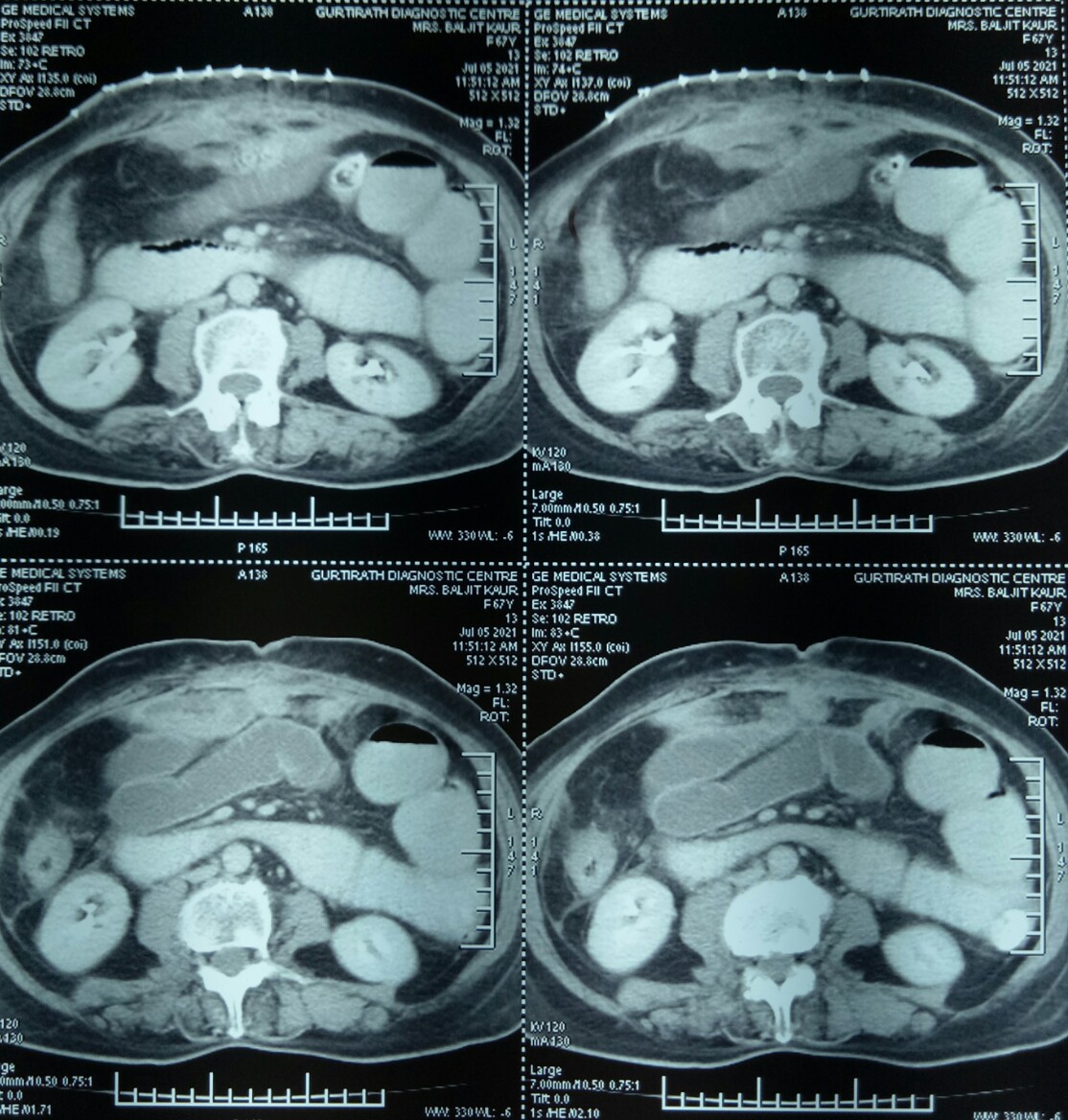
5.7.21 The abdomen was opened through midline incision for a full laparotomy and it was found there was a big mass of adherent small gut loops which could not be separated; hence the mass was excised and an end-to-end anastomosis (ileo-ileal) was performed.

This time she recovered very fast and very satisfactorily, passing stool and flatus on 2nd postoperative day, and started with oral intake 4th day onwards. Ready to be discharged home today (14.7.21).

July 23, 2021 at 10:51 am
Sir, was mesh used in the last/latest surgery or it was avoided I/v/o resection anastomosis?
LikeLike
July 25, 2021 at 2:46 pm
it was used; if one uses strict aseptic precautions, mesh can be used preventing recurrence of hernia which would have been more troublesome for the patient.
LikeLike