Archive for June 2021
Cervical polyp
Posted on: June 13, 2021
13.6.21
A big cervical polyp was removed along with the TAH and BLSOP (Dr Shalley’s case).

28.3.21
An obese man, Tejinder Singh (c/o Balwinder OTA) thought to have inguinal hernia gave great difficulties at inguinal exploration, the fluid of hydrocele present in the cord itself gave the appearance of a big direct or possibly sliding inguinal hernia and the cord dissection took a very long time. Eventually a small indirect sac was found but some more cord dissection led to a lot of fluid appearing in the field. It was all sucked out and the mesh repair performed. More than two months later the patient presented with a large hydrocele refilling and venereal warts on his prepuce and glans. So, after treatment of his genital warts, hydrocelectomy with epididymoorchiectomy had to be done on 23.6.21.
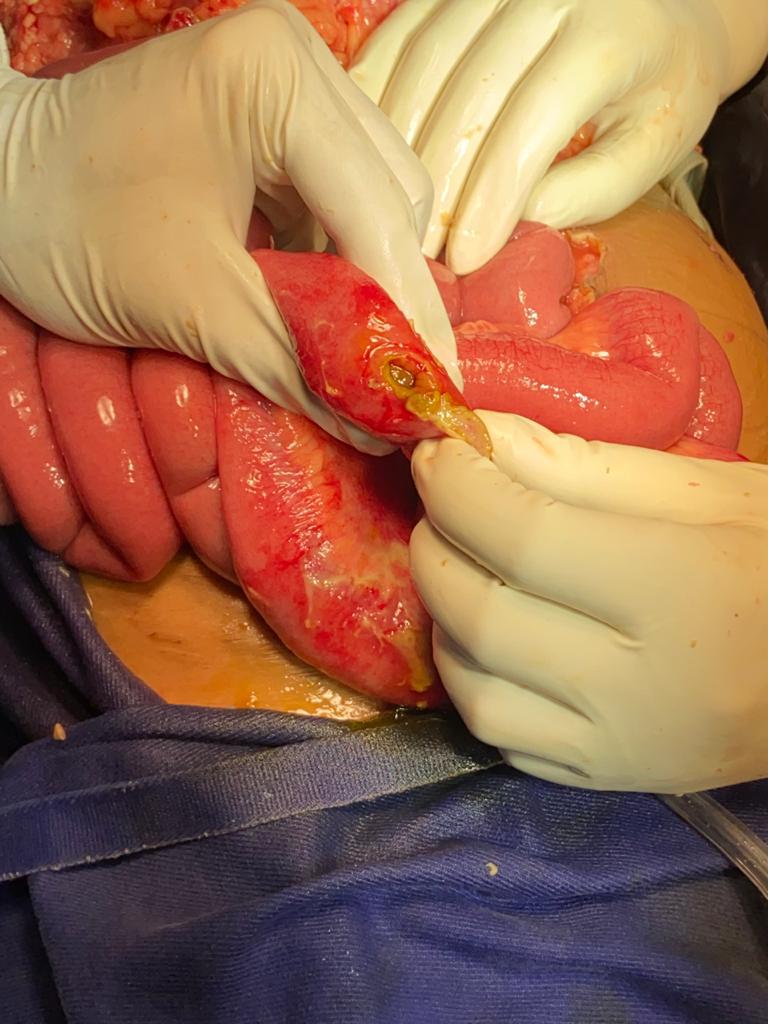
2.4.21
A monopolar diathermy small bowel injury during laparoscopic tubectomy (by gynae) about 5 days back resulted in peritonitis and gas under the diaphragm on x-rays. At urgent laparotomy by the assistant professor (Dr Abhishek), a thorough wash of the peritoneal cavity was done and the perforation exteriorized.
3.6.21
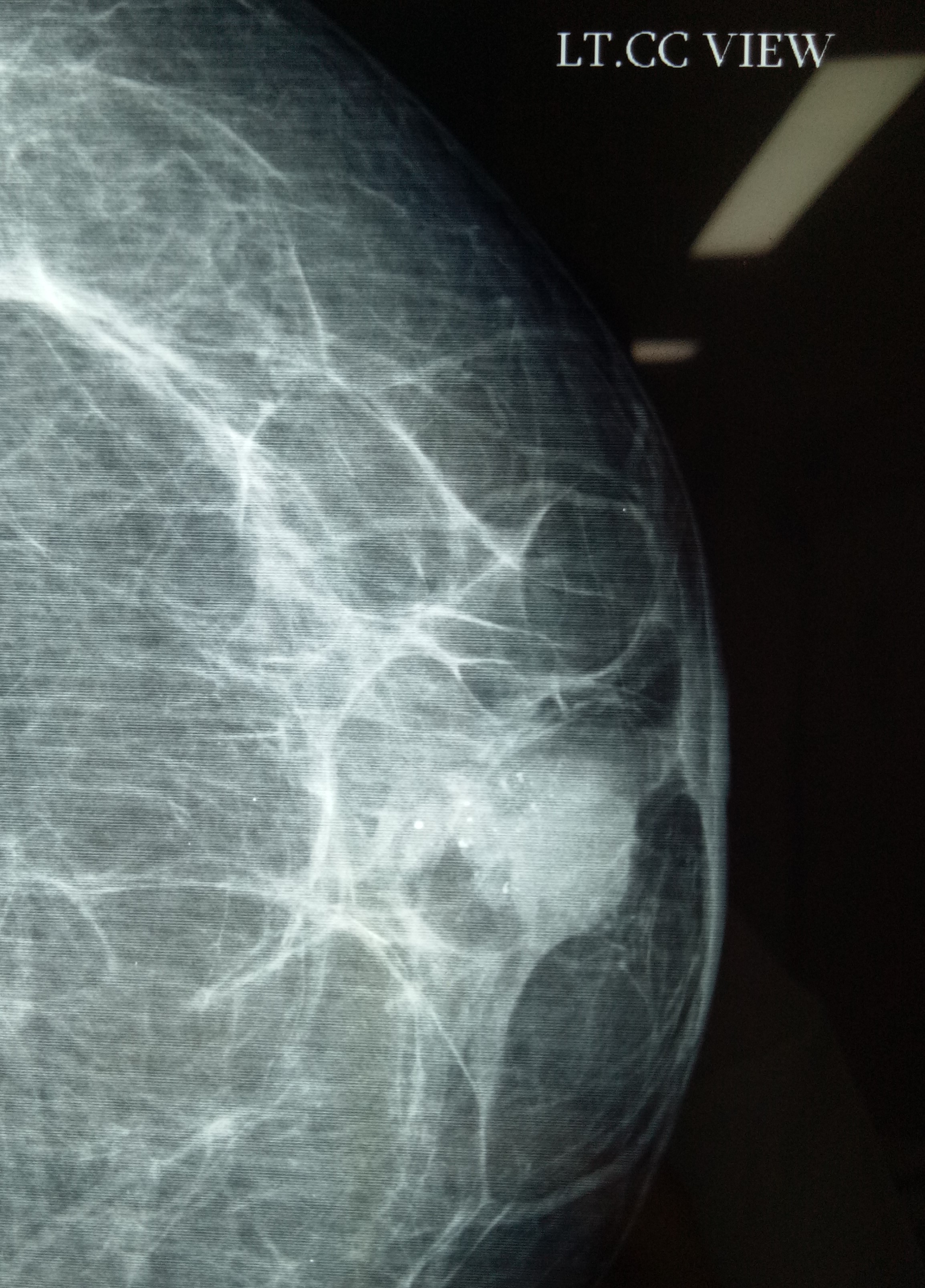
MRM for lobular carcinoma of breast (Dr Jagga’s case). Small tumor (less than 4 cm) and not expected to have metastases in axillary lymph nodes (which were not palpable) actually turned out to have a mass of several enlarged lymph nodes during axillary exploration.

18.10.20
An interesting encounter with gall stone disease: A 55 years old female (mother of Neetu, worker in OT of Shalley hospital), obese and diabetic and hypertensive was known to be carrying gall stones for many years. She landed up in septic shock (cholangitis) and severe pancreatitis and jaundice. Was luckily resuscitated and survived. An urgent ERCP (dr Atul) and stone extraction and stenting the bile duct followed. She reported passing her stent per rectum about 3 weeks later. Luckily the subsequent lap chole was not very difficult.
28.11.20
Another lesson in lap chole: an apparently easy lap chole (as per dr Jagga’s opinion) in a 55 years old female turned out to one of the most difficult and took more than 3 hours. First of all, the duodenum was adherent high up to the fundus which was very thick walled. This was carefully dissected safely. Next the cystic duct was thick walled and friable and the vicryl ligature cut through. Luckily the stump then could be clipped with two large clips. Thirdly, when beginning the dissection of the gall bladder it appeared as if the infundibulum was actually below where the cystic duct had been clipped. But by careful further dissection a safe plane behind the gall bladder could be created and what looked like the infundibulum was actually an large cystic lymph node (fallacy of perception).
Open CBDE
Posted on: June 13, 2021
27.7.20
Open cholecystectomy and CBD exploration after 4 failed attempts to clear the duct endoscopically, including two in the PGI.
5.9.20
An unusual encounter with a a femoral hernia in 60 years old male (s/o old retired laundry incharge RHP) who had been diagnosed as irreducible inguinal hernia. It actually turned out be not inguinal but femoral and mesh repair could be done through the inguinal incision itself.
7.10.20
A lap chole in a 45 years old male had to be converted due the the thick and big omental cake inseparably adherent to the thick walled gall bladder and duodenum. Even at open surgery, the procedure turned out to be very difficult due to dense adhesions around the Calot’s triangle.
16.10.20
Huge bilateral sliding inguinal hernias in an elderly gentleman (related to dr KD Singh, ex-principal GMC Patiala) who was carrying these hernias for more than 10 years. Took more than 2 hours for the bilateral mesh repair.
Locating an undescended testis laparoscopically, and a fallacy of perception in lap chole
Posted on: June 13, 2021
11.6.20
Called by dr Vikram while operating for right undescended testis in a 25 years old male but unable to find the testis in the inguinal canal.
The testis was easily located in the abdomen laparoscopically and removed laparoscopically through the inguinal incision already made.
22.7.20
An apparently easy lap chole became difficult due to two unforeseen problems – firstly due to the gall bladder being intrahepatic and secondly due to the small stones stuck in the fibrosed neck above which the gall bladder apparently narrowed down to the calibre of the cystic duct.
The first problem (the intrahepatic gall bladder) led to difficult and bloody dissection of the cystic artery which was eventually controlled. The second problem caused a fallacy of perception giving the appearance of the cystic duct to the infundibulum of the gall bladder. The dissection here too became very difficult and led to a tear in what was taken to be the cystic duct. A reappraisal of the thought process led to some dissection very low down and deep down to eventually find the real cystic duct just below the fibrosed neck of gall bladder with small impacted stones in it.
Just another example of visual fallacy of perception that so often causes trouble in lap chole.
