Archive for May 2016
Rectosigmoid cancer
Posted on: May 18, 2016
18.5.16
A huge ovarian cyst of the right ovary (with very little ovarian tissue salvageable) removed laparoscopically (Dr Karnail Singh’s case).
A rectosigmoid cancer resected by assistant professor Dr Walia, and specimen nicely photographed by a final year medical student.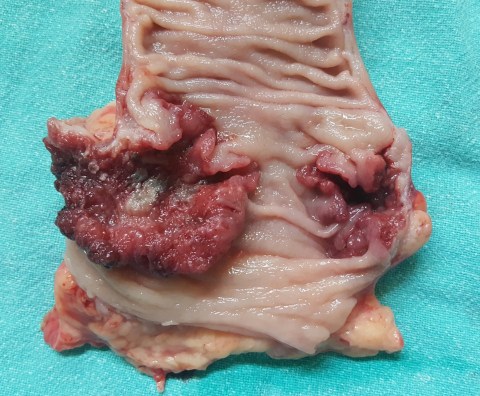
Familial adenomatous polyposis, a huge pseudocyst of pancreas and a choledochal cyst
Posted on: May 17, 2016
5.1.16 to 18.1.16 winter vacation
19.1.16: Following court orders, rechecked theory papers of PG students (who had failed and challenged their failure in court) at BFUHS, Faridkot along with dr Sushil Mittal.
28.1.16 court evidence at Amloh following the issuance of arrest warrants rather than the usual summons for expert witness.
24.2.16
A huge pseudocyst of pancreas in a 25 years old male, proved not to be a cystic neoplasm on investigations, managed by cystojejunostomy Roux-en-Y. The cyst was in the body and tail of pancreas, and parts of its wall had become gangrenous, and had to be excised.

5.3.16
An attempted TEP repair for bilateral inguinal hernias had to be converted to open due to poor relaxation and loss of space.
19.3.16
A choledochal cyst in a 55 years old female, managed by cyst excision and Roux-en-Y hepaticojejunostomy. An anastomotic leak developed and persisted for a long time.
9.4.16
Lap chole in a 62 years old retired doctor (sister of dr Bali, director health and family welfare, Punjab). Thick-walled gallbladder packed with stones. A cholecystohepatic duct appeared high up near the fundus, and was ligated as well as clipped.
12.4.16: Attended court at Dhuri, again following issuance of arrest warrants!

14.5.16
Total proctocolectomy and permanent ileostomy in a 42 years old poor man who had presented with rectal bleeding and severe anaemia, corrected by several blood transfusions. He had a family history of colorectal polyps and also had a duodenal polyp. The distalmost polyps were big and bleeding and possibly malignant and were present in the lower rectum, hence the decision to remove all of distal rectum and anus as well. An abdominoperineal resection and closure of anus were performed after total proctocolectomy was completed.


