Archive for November 2015
16.11.15
Multiple big fibroids in a 50 years old lady, causing pain and bleeding. Patient an unmarried jovial lady, and a close friend of Dr Geetanjali. Removed at a total abdominal hysterectomy (patient’s logical choice). She was in Dr Geetanjali’s office a few months later and while we were discussing fibroids remarked happily: “I had the mother of fibroids!”

18.11.15
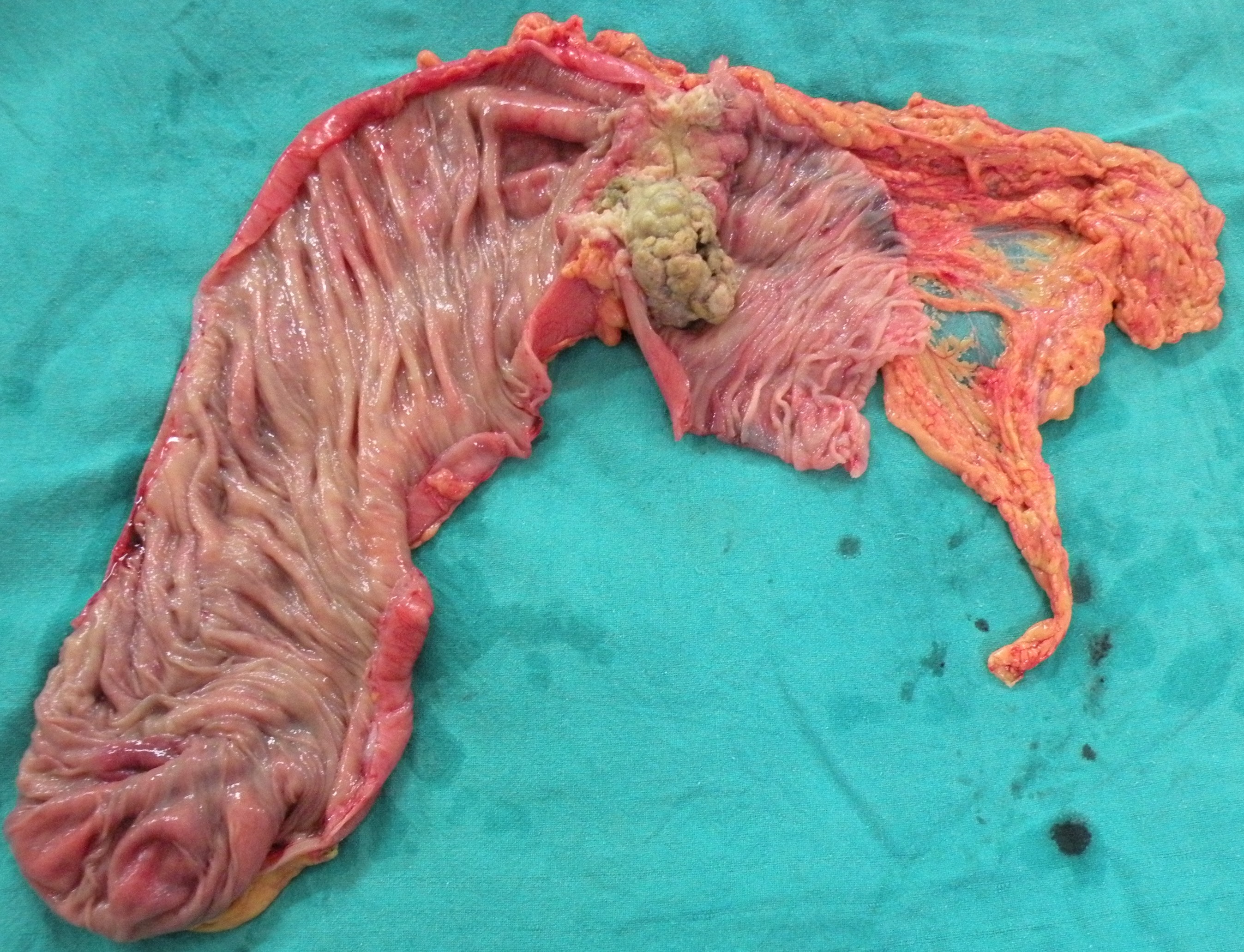
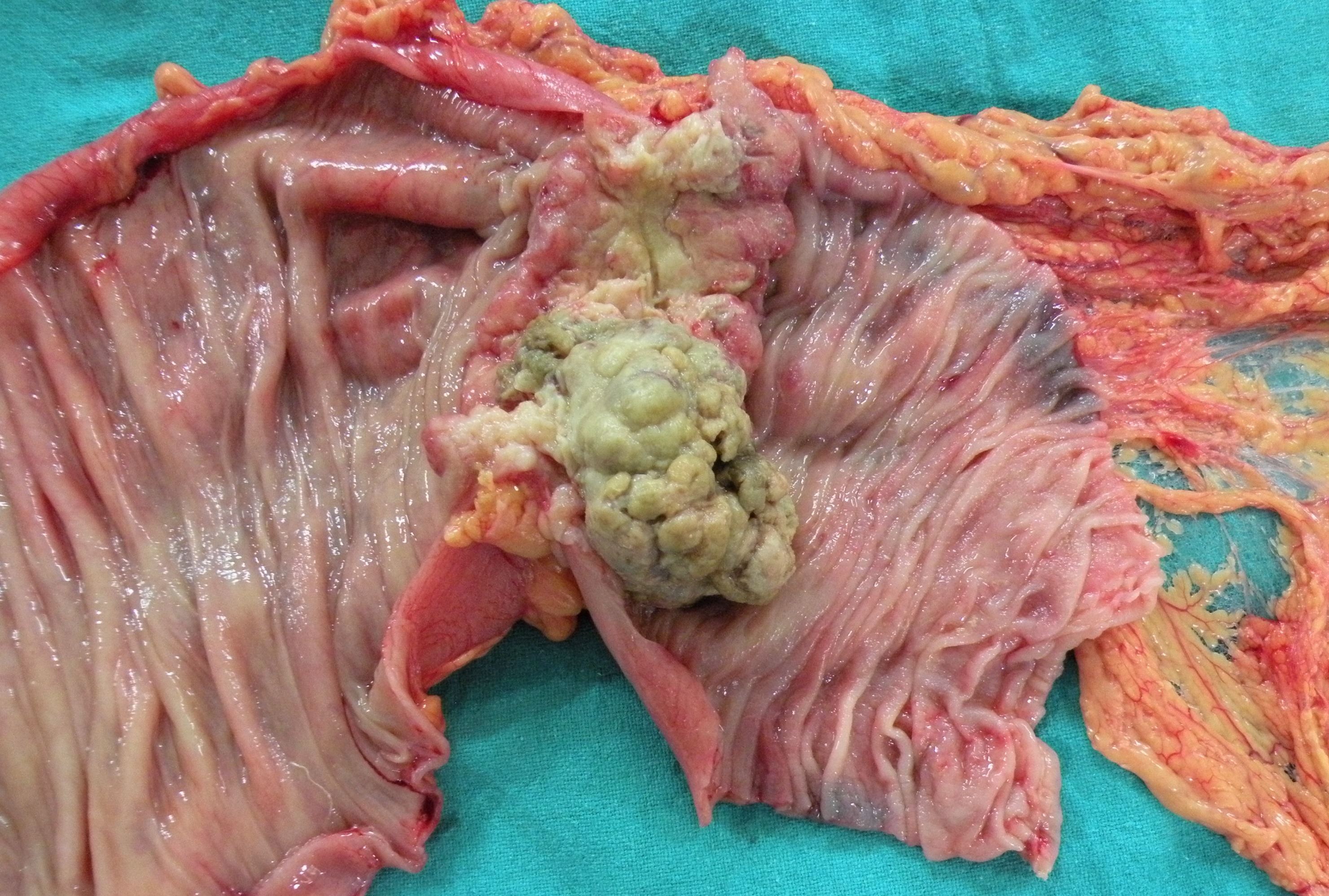
A distal radical gastrectomy in a 60 years old man (chronic smoker for a long time) for distal cancer causing gastric outlet obstruction. The tumor turned out to be bigger than expected (CT had only reported wall thickening of 2 cm), breaking through serosa and involving multiple lymph nodes above and below the pylorus, besides adhesions posteriorly with the pancreas. 

26.9.15
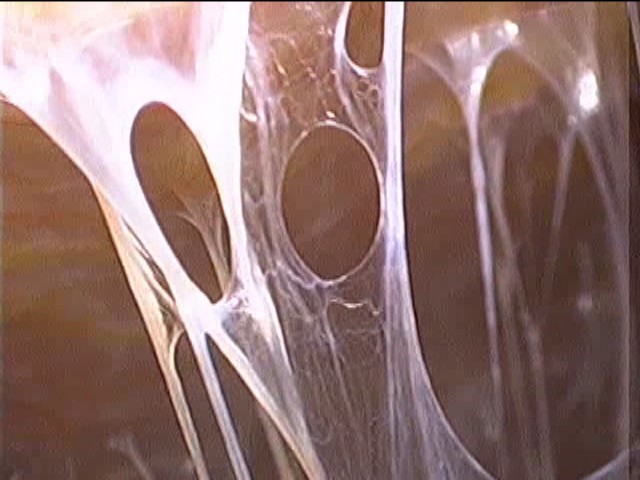
Dense adhesions around the liver and gall bladder, including violin-string type (Fitz-Hugh-Curtis), made lap chole difficult, but the procedure was eventually satisfactory.
Another lap chole (Angoori devi, c/o Kammo) was complicated by falling oxygen saturation levels near the end of the procedure. A C-arm image showed left pneumothorax, which necessitated a chest tube insertion and overnight stay in ICU for ventilation to expand the lung. The anesthetist’s explanation was the pneumothorax was due to diaphragmatic injury at surgery!
7.10.15
Visit to Chandigarh with dr Sushil Mittal for purchase of ETO sterilizers for operation theatres by the health systems corporation. Besides this purchase, another momentous decision was taken here. A suggestion given by dr Sushil Mittal was to stop using cars and instead use the bicycle for visits to the college and back. This proposal was immediately accepted and it was decided that both of us from now onwards will use bicycles rather than cars as far as possible.
18.10.15
Attended a CME on hepatobiliary and pancreatic surgery at Ludhiana (organised by dr Kuldeep Singh) along with dr Grover and Dr Jagga.
24.10.15
A laparotomy for abdominal pain and obstruction due to adhesions, following a traumatic bowel perforation which was treated in DMC with a resection-anastomosis and an ileostomy. This was followed by ileostomy closure, which was complicated by a fecal fistula, which had healed with conservative treatment. But the patient continued to experience pain and distension.
At exploration, extensive bowel adhesions had to be lysed, besides excising the ileo-cecal segment which was too densely adherent with an underlying thick-walled chronic abscess.

abscess cavity

ileum opened up with abscess cavity above
31.10.15
An intended Whipple resection for a cancer of the head of pancreas ended up in only a palliative biliary bypass procedure (cholecystojejunostomy). Once the pancreas was mobilized, the tumor in the head of pancreas was found to be densely adherent with the portal vein and also the gastroduodenal trunk (This was suggested by the CT scan, but still it was decided to go ahead with resection if possible).
4.11.15
An extended right hemicolectomy for a big palpable cancer in the transverse colon in a 60 years old female. The peglec bowel preparation by the residents had resulted in gross distension of all bowel proximal to the tumor, making surgery difficult and prolonged. However, the anastomosis with staples saved some time.