Archive for August 2014
Roux-en-Y duodenojejunostomy for SMA syndrome, a stricture at the lower end of ureter, a bad anal fistula, Harmonic lap choles, two wrong diagnoses, and a subtotal colectomy
Posted on: August 14, 2014
15.6.14
A wrongly diagnosed stone at lower end of ureter was found to have no stone, and actually a stricture for which the ureter was reimplanted into the bladder after excising the stricture. Dr Jagga’s case, a 7 years old male child.
8.7.14
A very bad chronic anal fistula with extensive suppuration and fibrosis all around the track, all of which had to be excised leaving a deep defect in the ischiorectal fossa, that eventually healed satisfactorily. Patient reported to be very happy! Had been suffering for long and had a couple of surgical attempts earlier.
28.7.14
2 lap choles done with Harmonic scalpel, neat and clipless division of the cystic duct performed for the thesis work of a resident.
31.7.14
A disappointing day.
A presumably easy lap chole for chronic cholecystitis turned out to have what looked like extensive intraperitoneal deposits and some ascites. Transverse colon was found to be densely adherent with the anterior abdominal wall making entry of subxiphoid port dangerous. The ascitic fluid was sampled and omentum biopsied. Cholecystectomy was deemed not possible. The biopsy report surprising came out to be tuberculosis!.
A young female (35 years old, HIV positive), had a mobile big intraperitoneal mass, reported on CT as ovarian (CA 125 also elevated). At operation the clinically mobile mass was found to be a mass in the greater omentum between the stomach and colon, but had a more extensive fixed retroperitoneal component posteriorly. Only a biopsy only was possible; and this was reported as sarcoma.
11.8.14
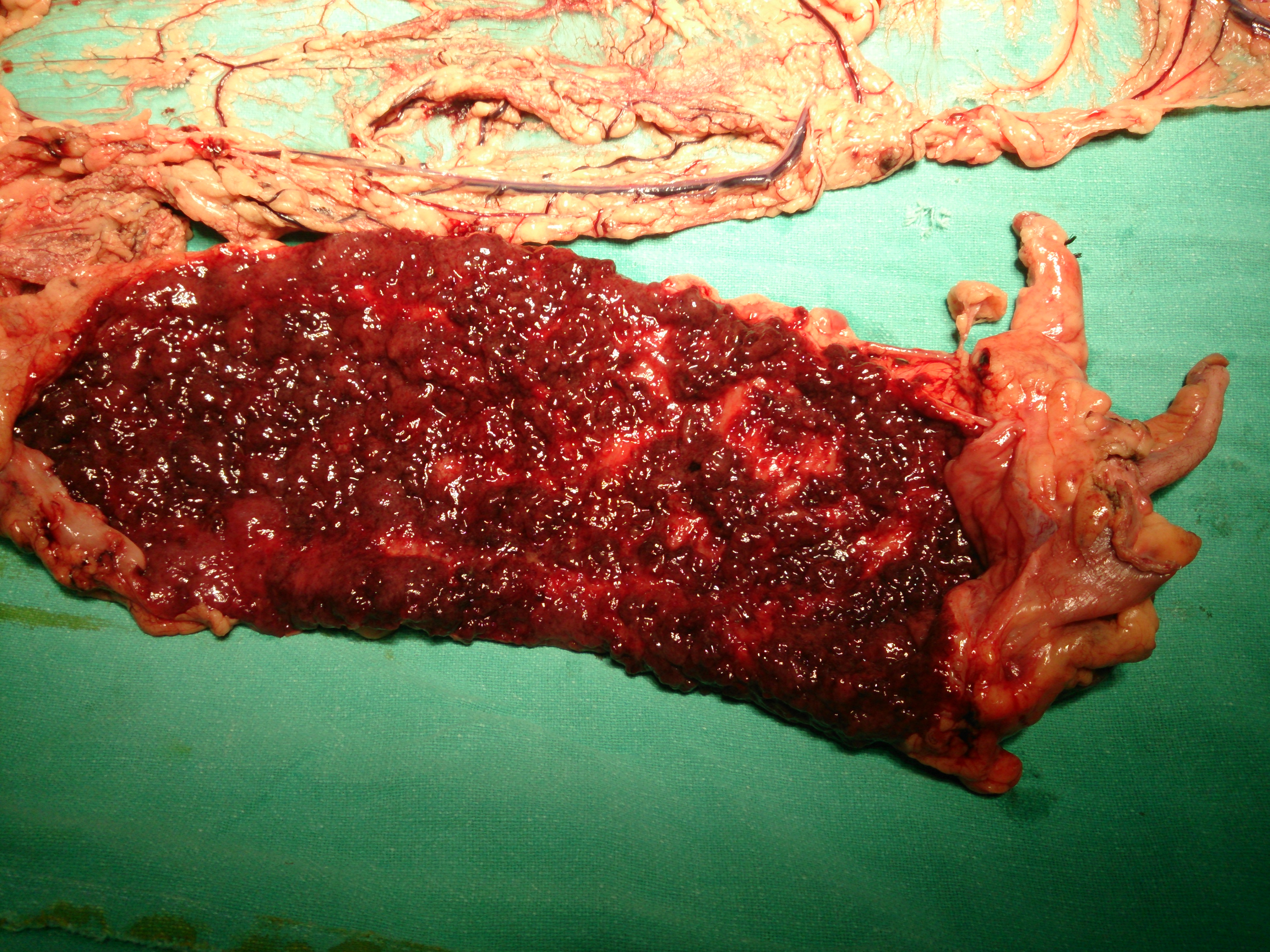
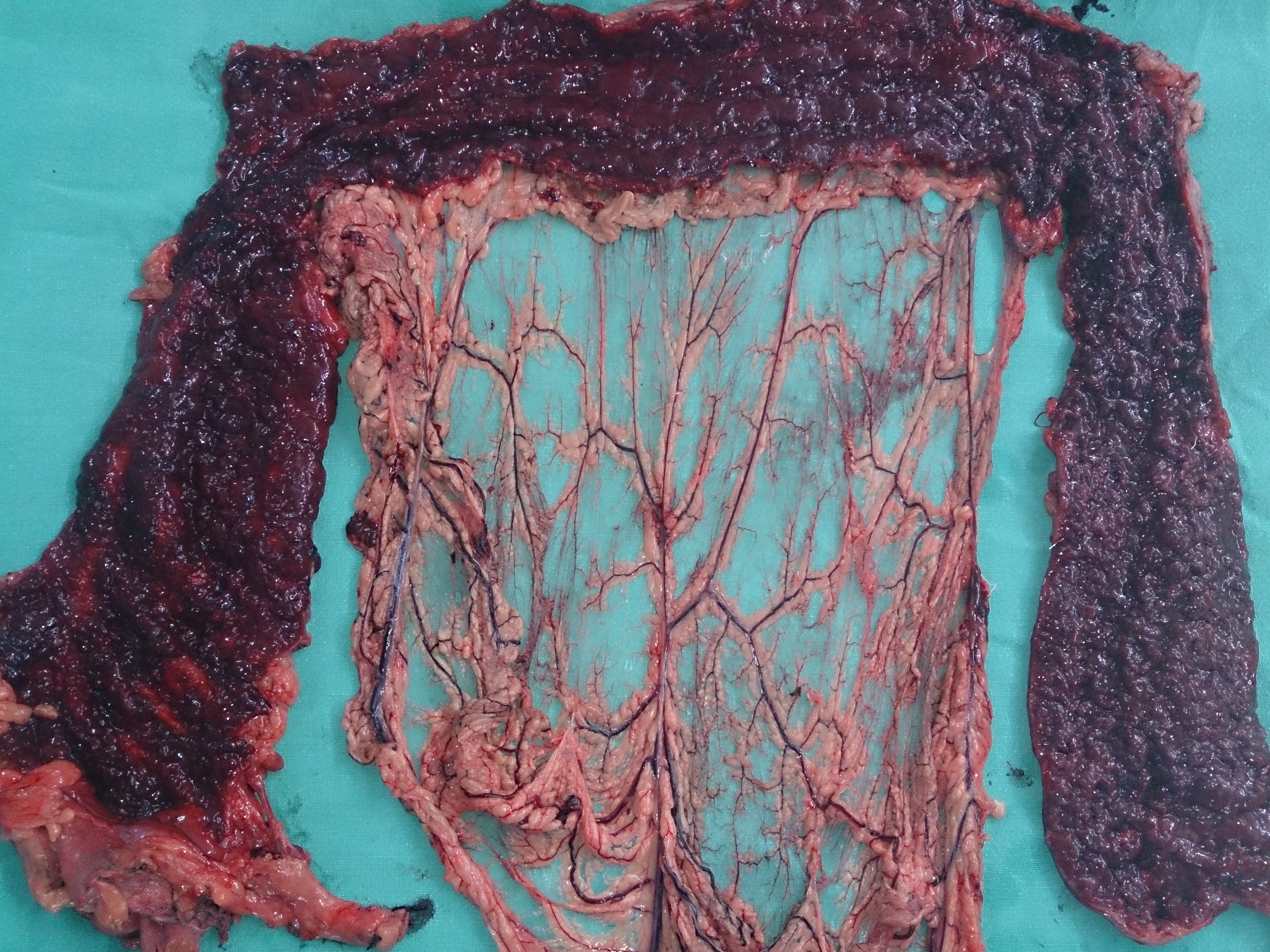
Subtotal colectomy and ileostomy for severe ulcerative colitis (pancolitis). Young (25 years old) patient, with fulminant ulcerative colitis, which had had remissions earlier, but now had actually become more severe, with the patient having developed abdominal pain, as well as increase in the number of bloody stools (now more than 10 per day). Referred from medical ward for surgery.

14.8.14
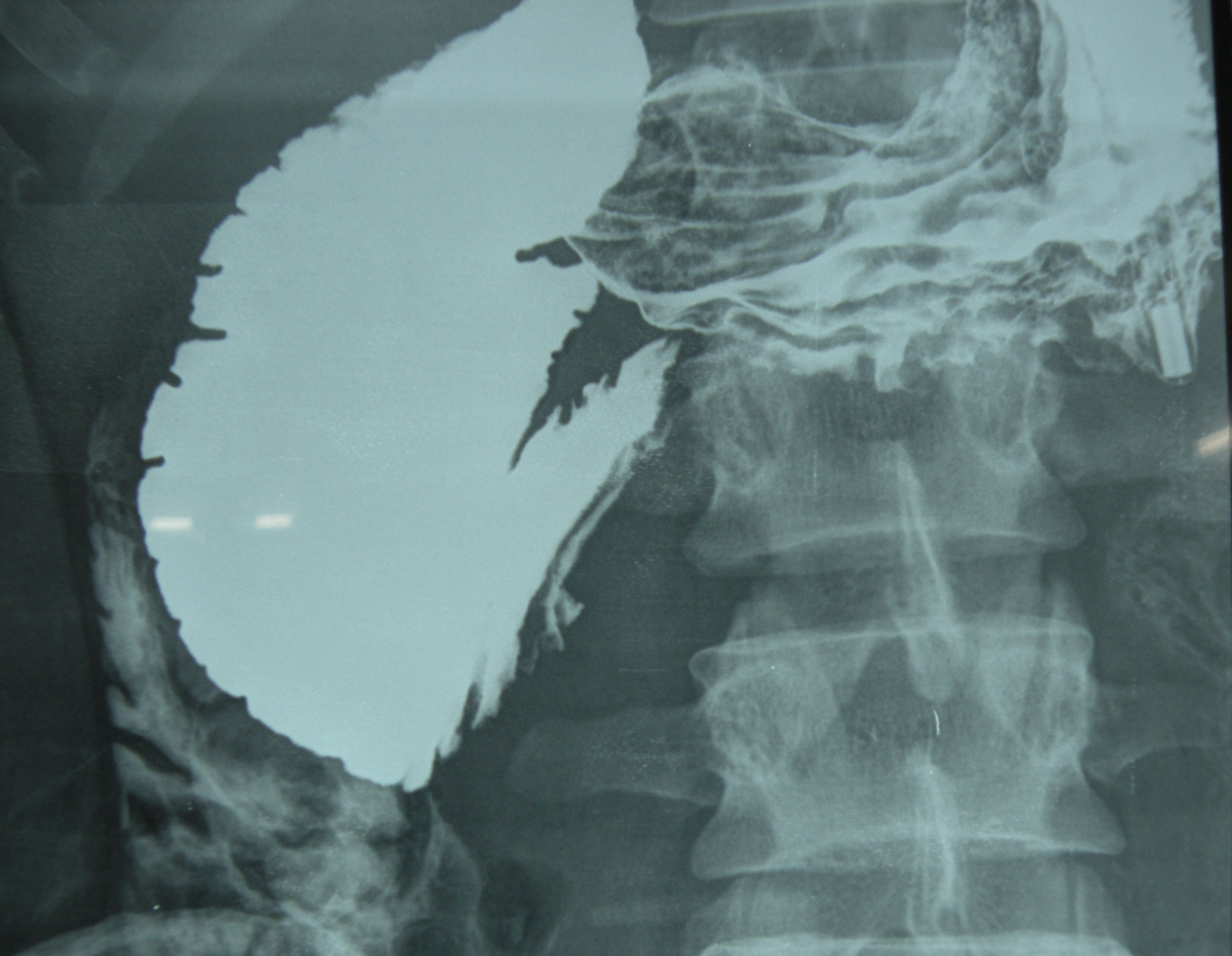
Roux-en-Y duodenojenunostomy for SMA syndrome. The young patient (27 years old) had undergone an appendicectomy (perhaps a wrong diagnosis) at Samana about two weeks back, but continued to have abdominal pain and vomiting. Barium study revealed a dilated duodenum up to the third part.
The angle between the aorta and SMA was 15 degrees on CT angiography.

At operation, after mobilizing the duodenum, the patient was found to have omental adhesions in the right lower abdomen ( at appendicectomy site). These were lysed. Interestingly, the upper small bowel had herniated through a hole created between the loops of proximal jejunum which were densely adherent to the posterior abdominal wall.
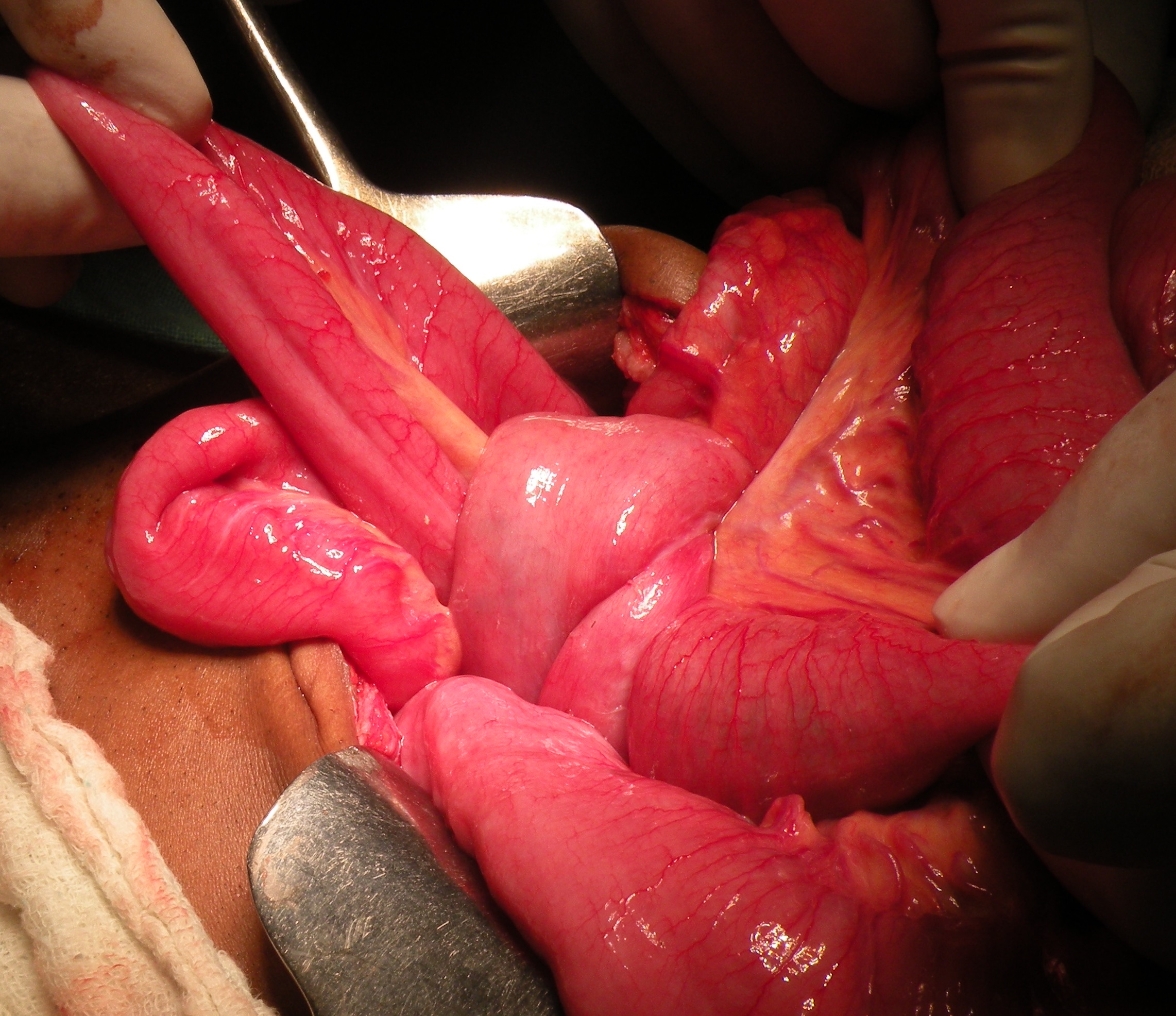
These adhesions were divided, and the jejunal loops released, only to find some stricturing in a loop at the site of adhesions. This upper jejunal loop was excised to remove the strictures and a Roux-en-Y DJ was made for cure of the SMA syndrome as well.
