Situs ambiguous(heterotaxia) with gall stones, an ileal carcinoid? and bad encounters with chronic liver disease
Posted on: October 11, 2013
9.9.2013
A lap chole converted due to impossible access (previous laparotomies for ileal perforation peritonitis, then closure of ileostomy + dense perihepatic adhesions).
18-20 September, 2013
Attended a SELSI conference at Srinagar. Good workshop showing hernias, lap ureterolithotomy, lap pyeloplasty, lap nephrectomy, lap CBD exploration.
23.9.13
Laparotomy for long-standing history of intermittent colicky abdominal pain in a 40 years old male. diagnosed presumptively with tuberculosis of intestines, and treated with ATT without relief. A recent CT showed 2 ileal strictures. At laparotomy, the segment of mid-ileum bearing the 2 strictures was excised and EEA done. Biopsy surprise was carcinoid.
26.9.13
Encounter with CLD 1 – A very difficult lap chole ended up in conversion. CLD with previously low PTI and previously postponed several times. Presently all LFTs and PTI reported to be normal. A very thick-walled and adherent gallbladder dissection resulted in duodenal tear and prolonged oozing from liver bed. After conversion to open, bleeding controlled with pressure and suture of liver bed, and the duodenal tear repaired. But the patient ended up in ICU due to incomplete recovery from anaesthesia, and there, her LFTs deteriorated and she died on 5th postop day.
7.10.10
Encounter with CLD 2 – A 50 years old female admitted with acute cholecystitis, now settled. Previously known history of portal hypertension and bleeding varices controlled with sclerotherapy for last 2 years. LFTs in normal range now – Childs grade A. So taken up for lap chole and burnt fingers again. Big vessels all around the gallbladder and in Calots triangle. Opened up for bleeding in Calots area, not controlled by pressure laparoscopically. At open operation too, the bleeding from liver bed severe, suturing of liver bed led to further bleeding, compounded by a retractor injury to the liver bed. 2 abdominal packs and pressure controlled the bleeding, and patient closed with packs in place. The packs were removed 5 days later when the patient stabilized, but the packs were found to be getting infected, thought the bleeding had stopped. The patient continued to drain through the abdominal drain for many more days.
10.10.13
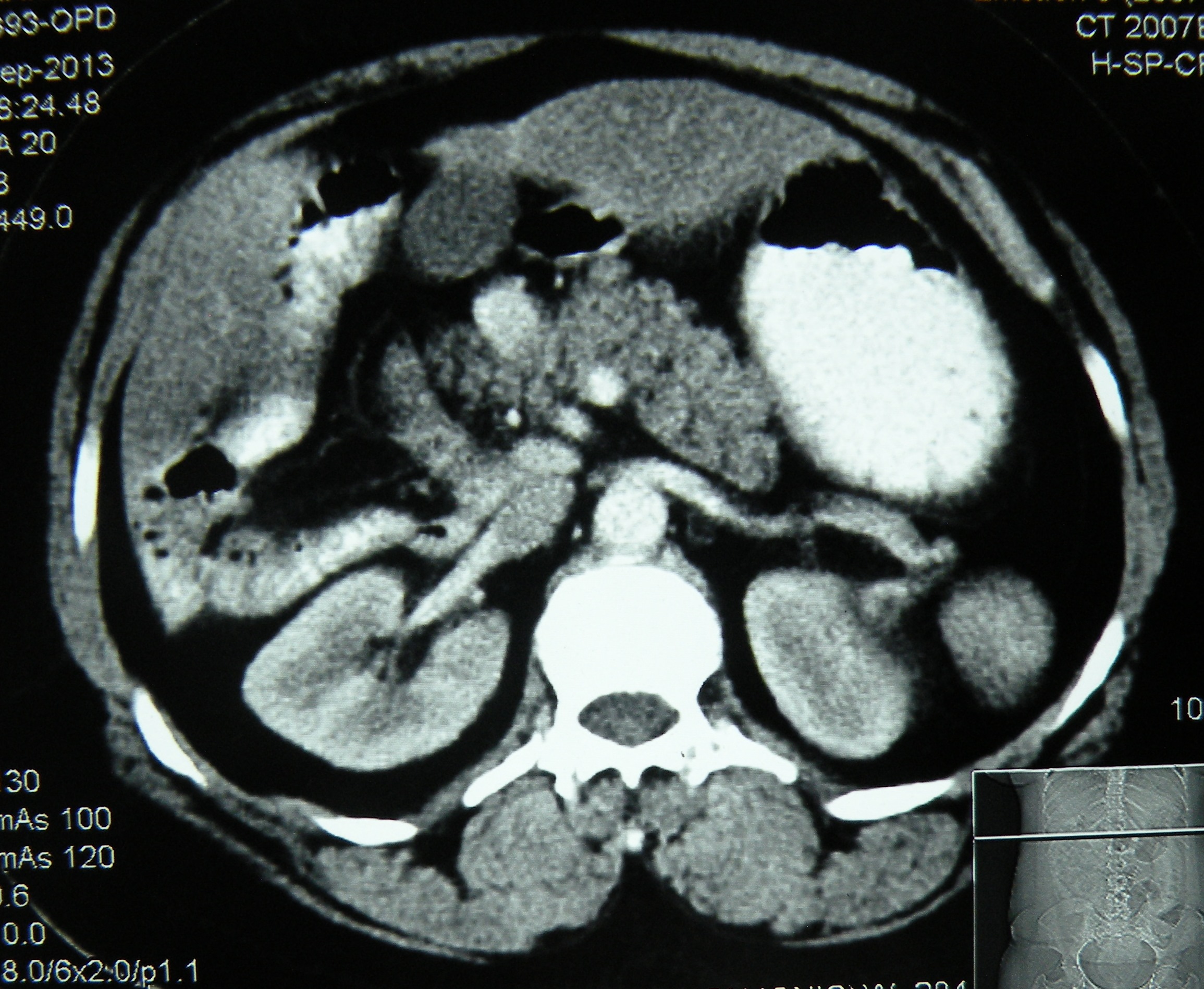
An interesting case of situs ambiguous (heterotaxic syndrome) presented with history of failed open attempt at civil hospital, Nabha to remove her gallbladder which could not be found by the surgeon. Imaging (US, CT, MRI) here showed a central liver, with gallbladder placed in the centre between the two lobes, polysplenia, truncated pancreas and dextrocardia. At surgery, the gall bladder was found just to the left of the falciform ligament. A difficult lap chole (due to dense adhesions with falciform ligament and omentum) was done, with the main operating port in the LUQ of the abdomen.

 published later in
published later in![]()
| CASE REPORT Year : 2014 | Volume : 4 | Issue : 3 | Page : 180–182 Laparoscopic cholecystectomy in situs ambiguous Anoop Varma1, Abhinav Mahajan1, Mohinder Singh1, Gunjeet S Sandhu1, Navkiran Kaur2, |

Leave a comment