Archive for August 2010
12.8.10
An epididymoorchiectomy on a 50 years old patient who had severe unremitting pain scrotum from choronic epidiymoorchitis, and wanted the operation. Biopsy reported as tuberculosis, and patient started on ATT.
13.8.10
Bilateral TEP repair for a recurred right inguinal hernia and a new one on the left side. The right side had an indirect as well as direct sac. The left side had a small indirect sac. After a long time, felt comfortable doing the TEP repair and enjoyed it too.



- In: operations
- 2 Comments
10.8.10
A direct right inguinal hernia in a 62 years old male (himself a doctor, an ENT specialist) repaired (Lichtenstein). Husband of dr Marwaha, retired professor of gynaecology.
A breast lump, an antibioma with thick walls and thick pus in it excised. A 25 years old from Nabha, with history of swelling in the breast for more than 2 months, treated with antibiotics. Besides the thick walled big abscess cavity which was excised, there were areas of tiny abscesses around the main abscess arising out of dilated ducts – duct ectasia. These were opened up too.

An external angular dermoid excised under general anaesthesia.



- In: operations
- 2 Comments
5.8.10
One of the most difficult lap choles so far, worth remembering. A 40 years old man had been admitted two weeks before with acute cholecystitis, treated conservatively and recovered to be sent home. However, he was admitted again as he felt he had never been really free from pain. Ultrasound revealed distended gallbladder and pericholecystic fluid. LFTs within normal range. At lap chole, dense omental adhesions had to be removed diligently before the gall bladder became visible. A grasp at the fundus tore the gall bladder to reveal thick pus which was aspirated, and along with this came out a cast of a fibrinous wall of the abscess. Slow dissection led to the big Hartmann pouch the grasping of which was impossible due to the big stone stuck in it. This was opened up, the stone retrieved, broken into pieces to remove it piecemeal, and then only the neck of the gall bladder became clear. Further dissection of the area was deemed dangerous, and the neck was ligated with vicryl 1 twice with extracoporeal knots. Thereafter, separating the wall of the gall bladder from the liver bed was another difficult task, so some of the wall was left behind with the liver, and cauterised. Removal of the big thickwalled gallbladder was not possible in one piece, so it was divided in steps into 4 pieces, each one being removed separately. The whole procedure took nearly 4 hours, but in the end was a satisfying one. Next day the patient was smiling but the surgeon aching all over.
6.8.10
Anothe difficult lap chole, but not like yesterday’s. Male patient again.
AndersonHynes pyelopasty in a young (25) female, big hydronephrotic right kidney, with 29% function on DTPA scan.
A perianal fistula, starting from under the urethra with three openings and ending near the anal verge blindly. All tracks excised.
23.6.10
A laparotomy for dense ileal adhesions stuck in pelvis following TAH 10 days back. Lysis of adhesions, however, did not work and had to be reexplored to do REEA a few days later.
25.6.10
GOMCO 75 batch meeting at dr Zora singh’s place Chandigarh.
26.6.10
TEP reapir for RIH
6.7.10
saw dr grover recovering after CABG at fortis, mohali
9.7.10
TLH : The urinary bladder got injured, repaired.
13.7.10
35 years old female with a big hydatid cyst posterior right liver. Partial cystectomy and omentoplasty after excision of cyst walls.
15.7.10
A big left parotid swelling, difficult parotidectomy, facial nerve in the tumour, sacrificed. Biopsy reported as lymphoma!
20.7.10
Orchidopexy for undescended testis located at the internal ring. 10 years old child from Patran. IE vessels divided to gain length.
30.7.10
A paratidectomy, mixed parotid tumour, facial nerve nicely displayed and protected.
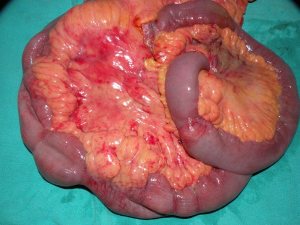
3.8.10
A planned right hemicolectomy became extensive resection of distal ileum and right colon. A 35 years old female admitted with a mass in right iliac fossa not resolving. CT showed a long tubular stricture in the whole of right colon, The mass regresses somewhat with conservative treatment. A barium enema showed a tight stricture reportedly in the right colon. At exploration, multiple strictures in the terminal ileum and some palpable thickening in the right colon, all of which was excised.




{kind=link}